Department of Molecular and Clinical Pharmacology, University of Liverpool, United Kingdom.
Department of Biostatistics, University of Liverpool, United Kingdom.
Clin Infect Dis. 2020 May 6;70(10):2062-2072. doi: 10.1093/cid/ciz589.
Combination antiretroviral therapy results in metabolic abnormalities which increase cardiovascular disease risk. We evaluated whether telmisartan reduces insulin resistance in human immunodeficiency virus (HIV)-positive individuals on antiretrovirals.
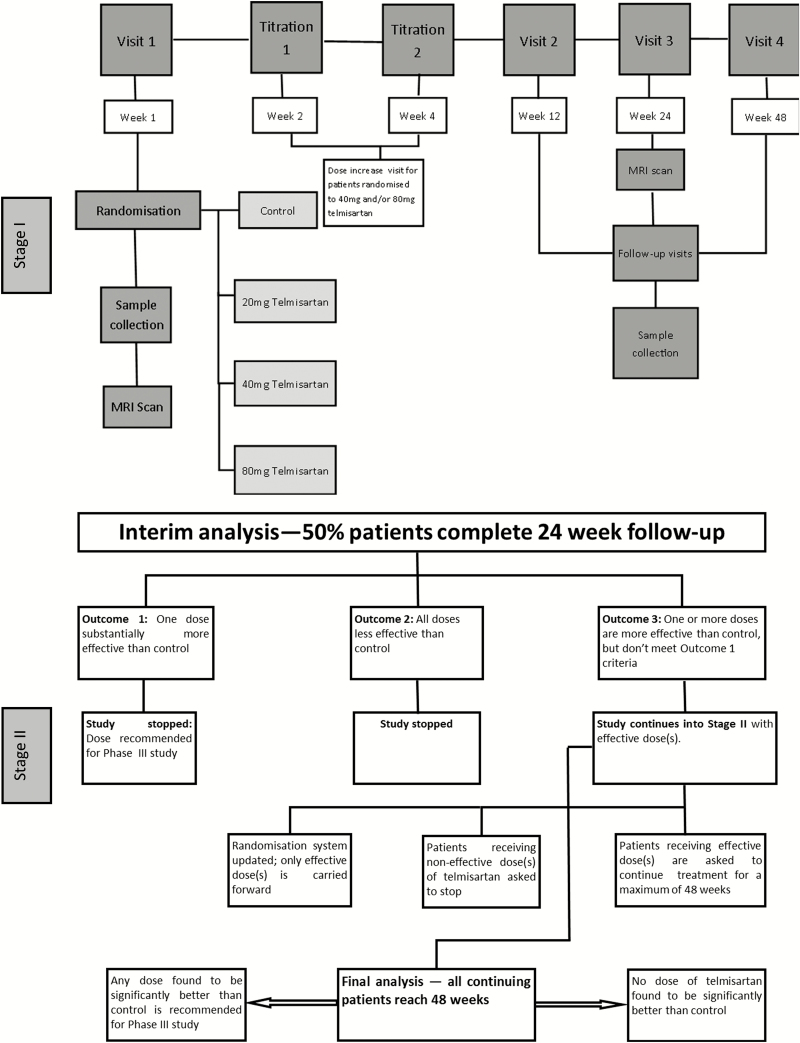
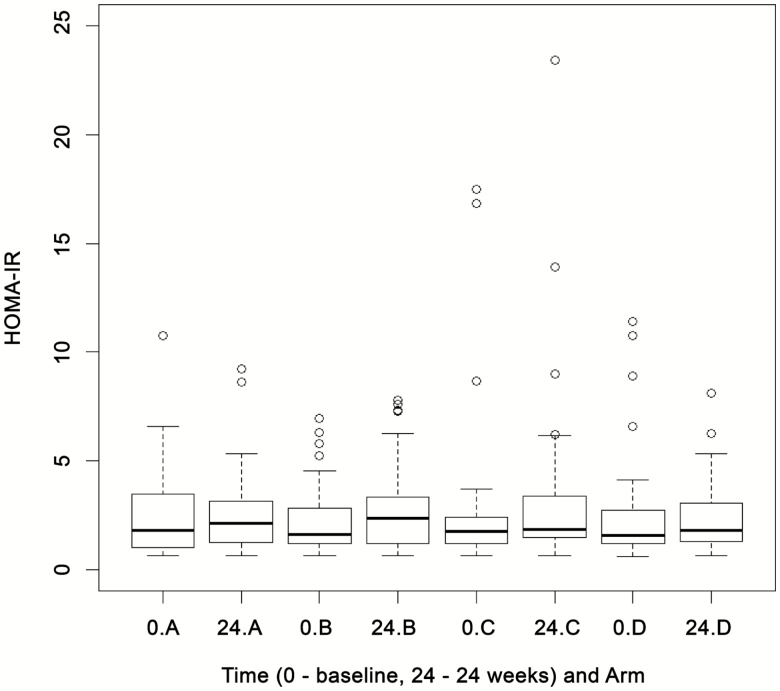
We conducted a multicenter, randomized, open-label, dose-ranging controlled trial of telmisartan. Participants with HIV infection receiving combination antiretroviral therapy were randomized equally to either no intervention (control) or 20, 40, or 80 mg telmisartan once daily. The adaptive design allowed testing of all dose(s) of telmisartan in stage I, with the promising dose(s) being taken into stage II. The primary outcome measure was reduction in homeostasis model assessment of insulin resistance (HOMA-IR) at 24 weeks.
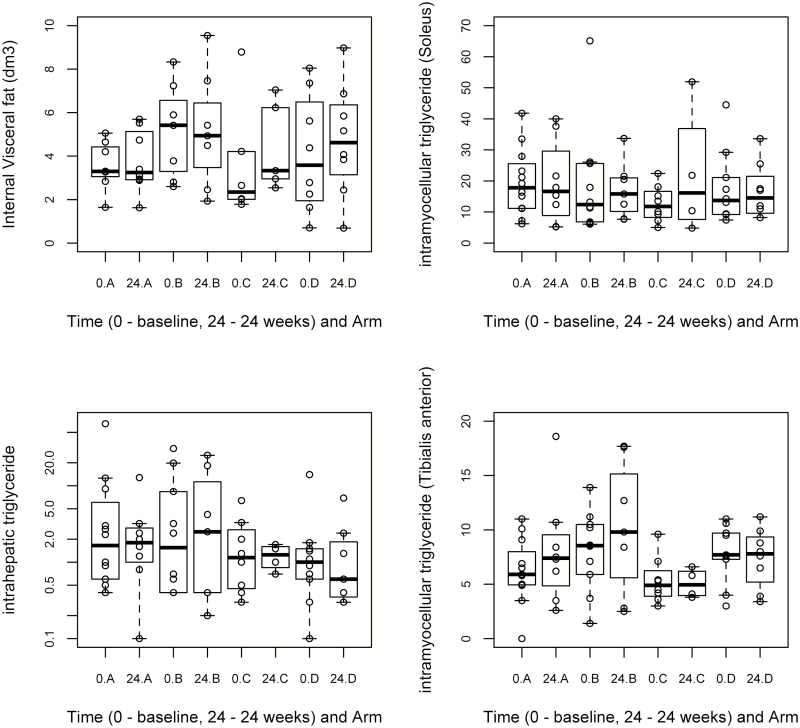
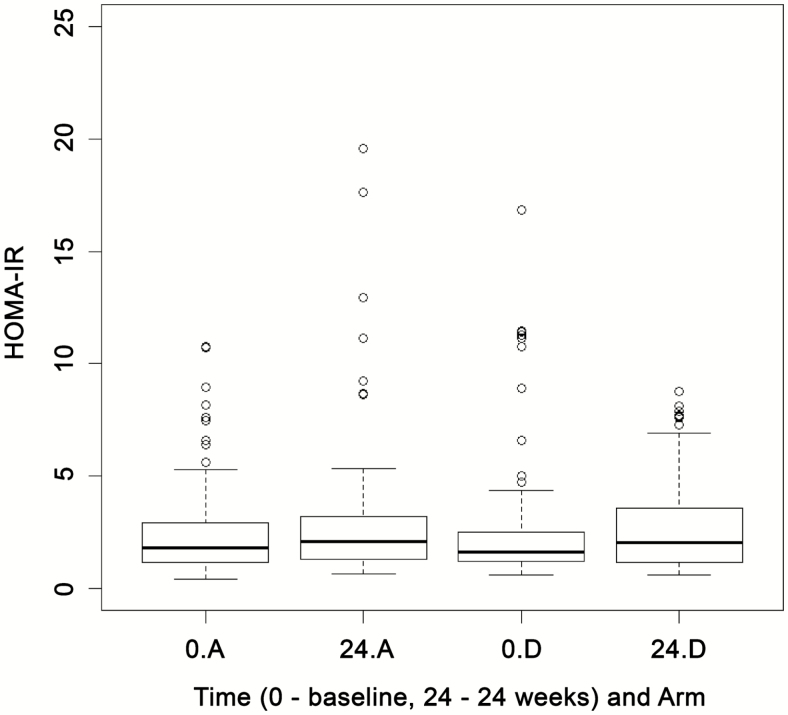
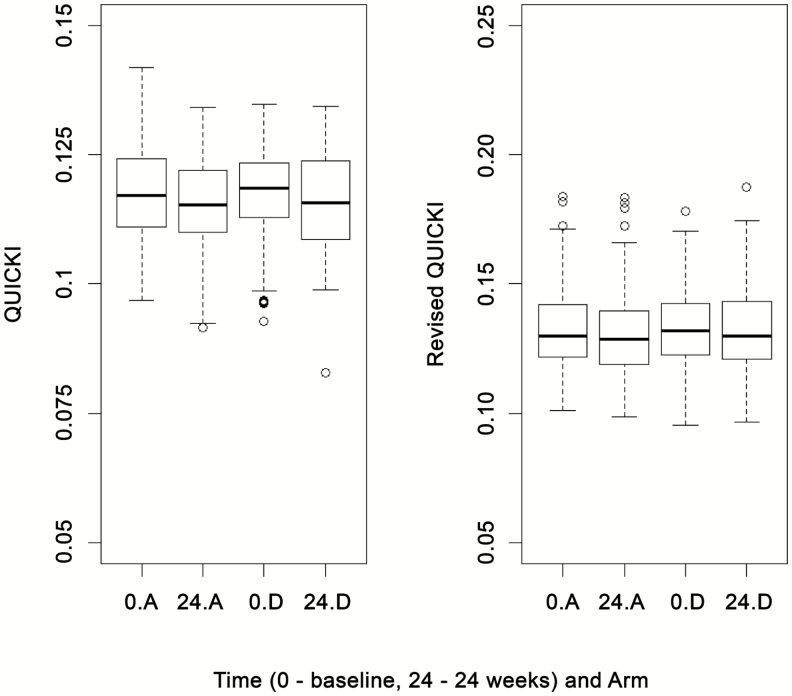
A total of 377 patients were recruited. In stage I, 48, 49, 47, and 45 patients were randomized to control and 20, 40, and 80 mg telmisartan, respectively (total n = 189). At the interim analysis, 80 mg telmisartan was taken forward into stage II. At the end of stage II (n = 105, control; 106, 80-mg arm), there were no differences in HOMA-IR (estimated effect, 0.007; SE, 0.106) at 24 weeks between the telmisartan (80 mg) and nonintervention arms. Longitudinal analysis over 48 weeks showed no change in HOMA-IR, lipid or adipokine levels. There were significant (P ≤ .05), but marginal, improvements in revised Quantitative Insulin Sensitivity Check Index (QUICKI) (0.004) and plasma hs-CRP (-0.222 mg/L) and reduction in liver fat content (1.714 mean reduction; P = .005).
No significant effect of telmisartan was demonstrated on the primary outcome (HOMA-IR), but there were marginal improvements with some secondary outcome measures. Further studies in this population are warranted to identify novel strategies for preventing cardiovascular morbidity and mortality.
ISRCTN registry (51069819).
联合抗逆转录病毒疗法会导致代谢异常,从而增加心血管疾病的风险。我们评估了替米沙坦是否能降低接受抗逆转录病毒药物治疗的艾滋病毒(HIV)阳性个体的胰岛素抵抗。
我们进行了一项多中心、随机、开放标签、剂量范围对照试验,评估替米沙坦。接受联合抗逆转录病毒治疗的 HIV 感染患者被平均随机分为无干预(对照组)或每日服用 20、40 或 80mg 替米沙坦。适应性设计允许在第一阶段测试所有替米沙坦剂量,有前途的剂量进入第二阶段。主要结局测量是 24 周时稳态模型评估的胰岛素抵抗(HOMA-IR)的降低。
共招募了 377 名患者。在第一阶段,48、49、47 和 45 名患者被随机分为对照组和 20、40 和 80mg 替米沙坦组(共 189 名患者)。在中期分析时,80mg 替米沙坦进入第二阶段。在第二阶段结束时(n=105,对照组;n=106,80mg 组),替米沙坦(80mg)与非干预组之间 24 周时 HOMA-IR 无差异(估计效应,0.007;SE,0.106)。48 周的纵向分析显示 HOMA-IR、血脂或脂肪因子水平无变化。修订后的定量胰岛素敏感性检查指数(QUICKI)(0.004)和血浆 hs-CRP(-0.222mg/L)有显著(P≤0.05)但边缘改善,肝脂肪含量降低(平均减少 1.714;P=0.005)。
替米沙坦对主要结局(HOMA-IR)没有显著影响,但一些次要结局有轻微改善。需要在该人群中进行进一步的研究,以确定预防心血管发病率和死亡率的新策略。
ISRCTN 注册(51069819)。