Radiology, Massachusetts General Hospital, White 270 | 55 Fruit Street, Boston, 02114, USA.
Department of Radiology and Imaging Sciences, Indiana University School of Medicine, 550 N. University Blvd. Suite 0663, Indianapolis, IN, 46202, USA.
Abdom Radiol (NY). 2020 May;45(5):1420-1438. doi: 10.1007/s00261-019-02191-0.
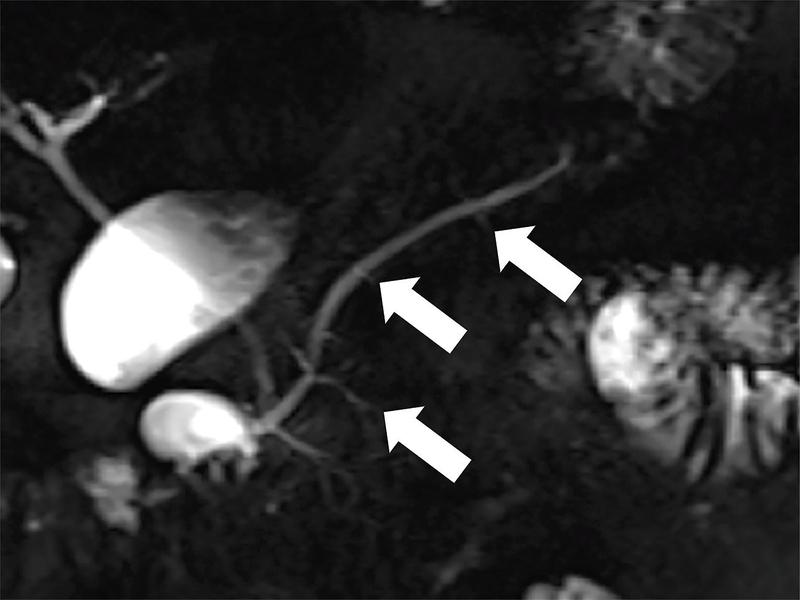
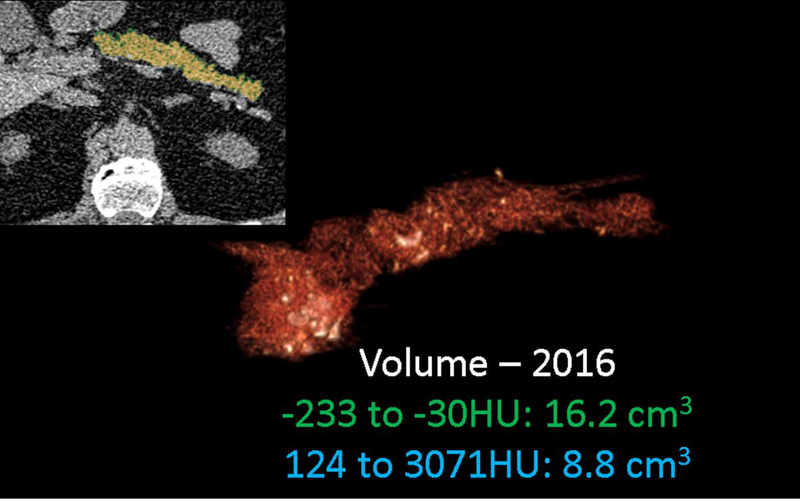
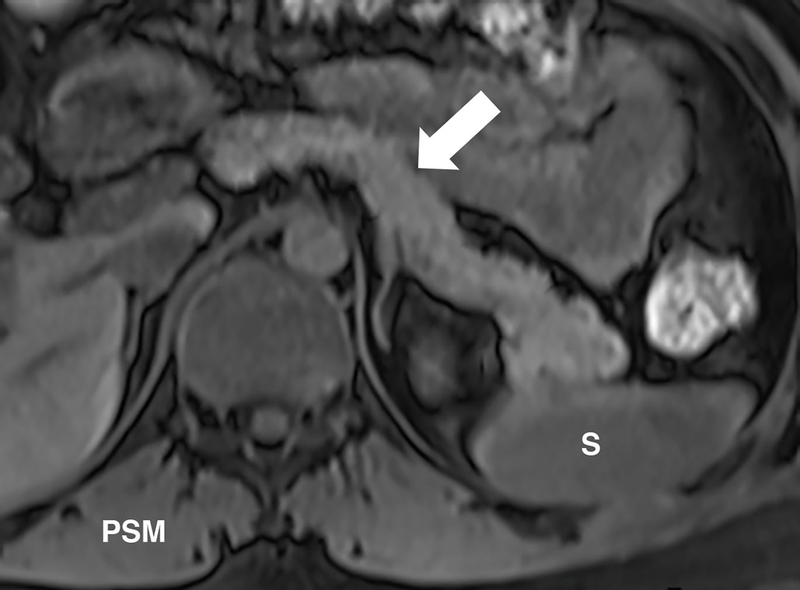
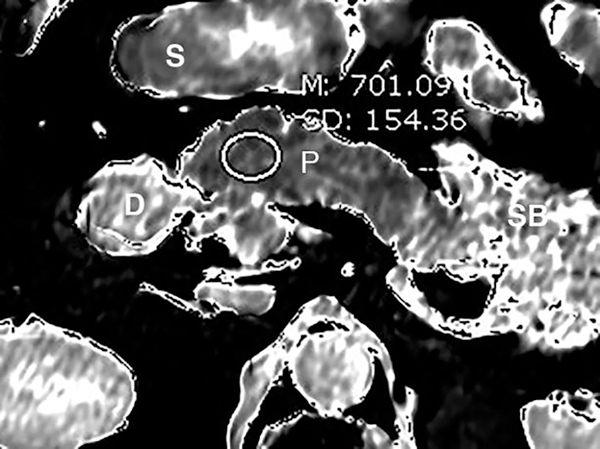
MRI and MRCP play an important role in the diagnosis of chronic pancreatitis (CP) by imaging pancreatic parenchyma and ducts. MRI/MRCP is more widely used than computed tomography (CT) for mild to moderate CP due to its increased sensitivity for pancreatic ductal and gland changes; however, it does not detect the calcifications seen in advanced CP. Quantitative MR imaging offers potential advantages over conventional qualitative imaging, including simplicity of analysis, quantitative and population-based comparisons, and more direct interpretation of detected changes. These techniques may provide quantitative metrics for determining the presence and severity of acinar cell loss and aid in the diagnosis of chronic pancreatitis. Given the fact that the parenchymal changes of CP precede the ductal involvement, there would be a significant benefit from developing MRI/MRCP-based, more robust diagnostic criteria combining ductal and parenchymal findings. Among cross-sectional imaging modalities, multi-detector CT (MDCT) has been a cornerstone for evaluating chronic pancreatitis (CP) since it is ubiquitous, assesses primary disease process, identifies complications like pseudocyst or vascular thrombosis with high sensitivity and specificity, guides therapeutic management decisions, and provides images with isotropic resolution within seconds. Conventional MDCT has certain limitations and is reserved to provide predominantly morphological (e.g., calcifications, organ size) rather than functional information. The emerging applications of radiomics and artificial intelligence are poised to extend the current capabilities of MDCT. In this review article, we will review advanced imaging techniques by MRI, MRCP, CT, and ultrasound.
MRI 和 MRCP 通过对胰腺实质和胰管成像在慢性胰腺炎(CP)的诊断中发挥重要作用。由于 MRI/MRCP 对胰管和腺体变化的敏感性增加,因此比计算机断层扫描(CT)更广泛地用于轻度至中度 CP;然而,它无法检测到晚期 CP 中可见的钙化。定量磁共振成像相对于传统定性成像具有潜在优势,包括分析的简便性、定量和基于人群的比较,以及对检测到的变化的更直接解释。这些技术可能为确定腺泡细胞丢失的存在和严重程度提供定量指标,并有助于慢性胰腺炎的诊断。鉴于 CP 的实质变化先于胰管受累,因此从开发基于 MRI/MRCP 的更稳健的诊断标准中获益匪浅,该标准结合了胰管和实质发现。在各种横断面成像方式中,多排 CT(MDCT)自出现以来一直是评估慢性胰腺炎(CP)的基石,因为它无处不在,可评估主要疾病过程,以高灵敏度和特异性识别假性囊肿或血管血栓形成等并发症,指导治疗管理决策,并在几秒钟内提供各向同性分辨率的图像。传统的 MDCT 具有一定的局限性,主要用于提供形态学信息(例如钙化、器官大小),而不是功能信息。放射组学和人工智能的新兴应用有望扩展 MDCT 的现有功能。在这篇综述文章中,我们将回顾 MRI、MRCP、CT 和超声的先进成像技术。