Division of Pain Medicine, Department of Anesthesiology, Intensive Care and Pain Medicine, University of Helsinki and Helsinki University Hospital, Helsinki, Finland.
Folkhälsan Research Center, Helsinki, Finland.
PLoS One. 2019 Aug 20;14(8):e0221437. doi: 10.1371/journal.pone.0221437. eCollection 2019.
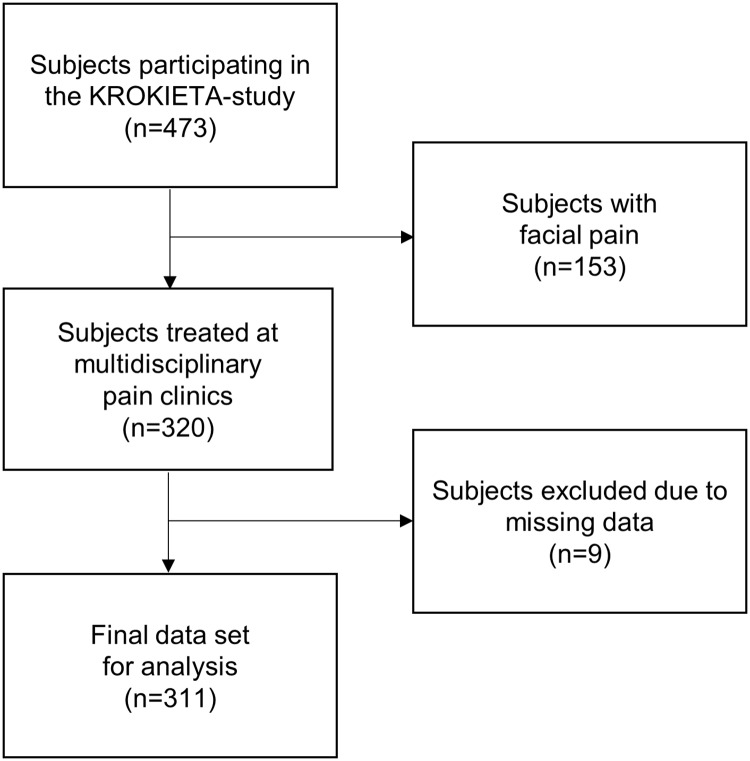
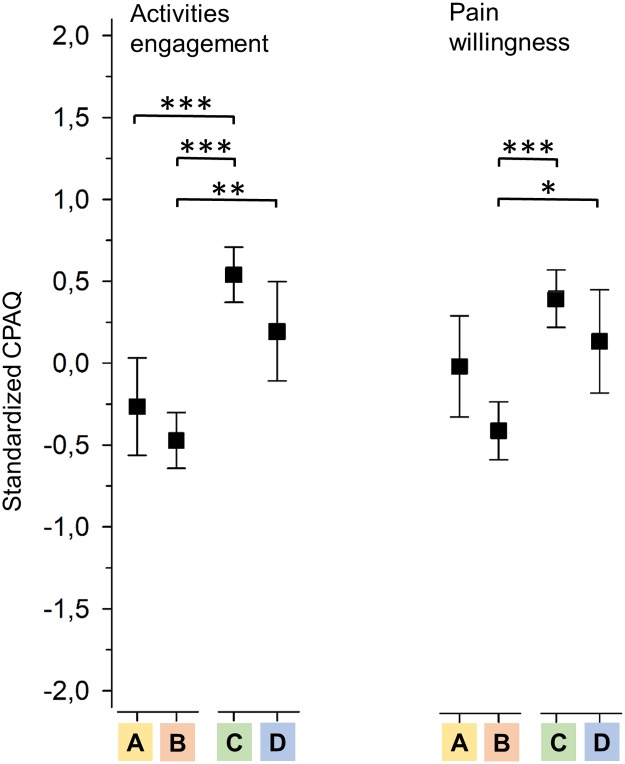
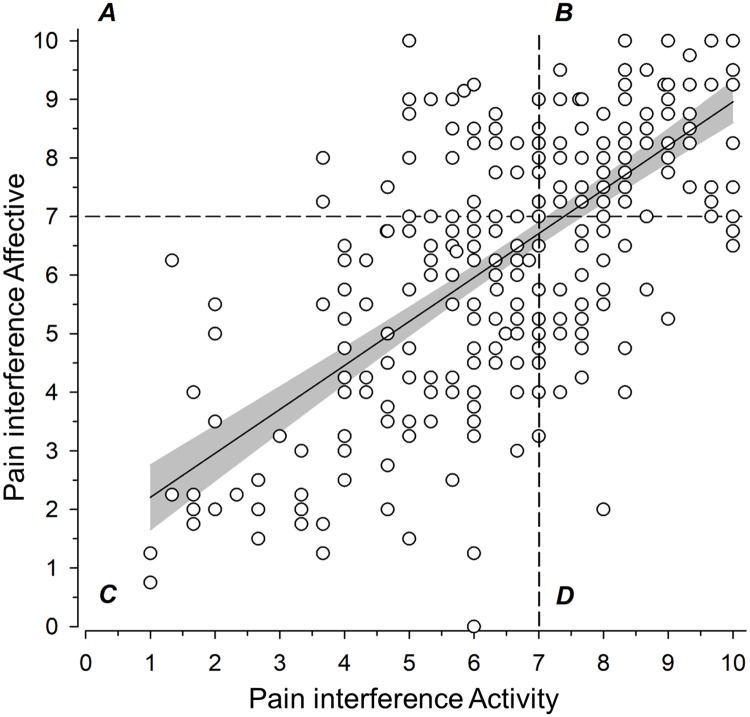
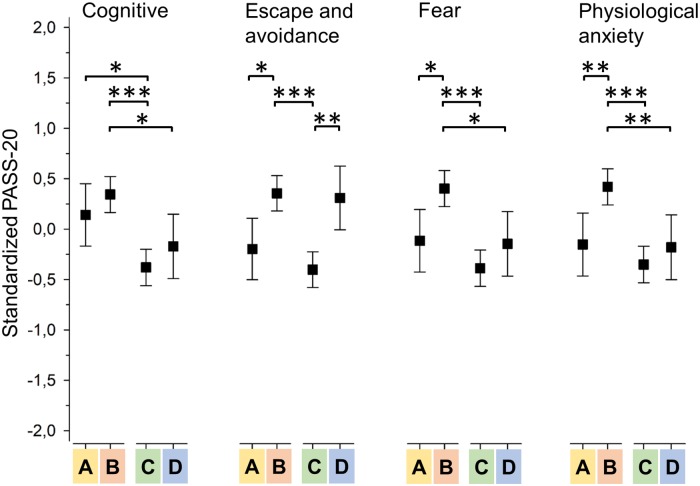
Chronic pain patients enter treatment with different problem profiles making careful assessment a necessity for more individualized treatment plans. In this cross-sectional study we assigned 320 patients entering tertiary multidisciplinary pain treatment into four categories based on whether they scored low or high on the activity and the affective pain interference dimensions of the Brief Pain Inventory (BPI). To determine whether this categorization system delineates issues that should be assessed further, the categories were compared with ANOVA and MANOVA analyses on three domains: variables affecting physical well-being (body mass index, exercise, substance use), psychological resources (mood), and pain-specific psychological factors (pain anxiety, pain acceptance). The results indicated that subjects who scored low on both interference dimensions compared similarly in weight: mean Body Mass Index (BMI) 27.0 (SD 6.0) kg/m2, and exercise: mean of 2.4 (SD 1.7) exercising sessions over 20 minutes per week, to the general population, had no depressive symptoms on average: mean Beck Depression Index II (BDI-II) score 11.7 (SD 7.5), and had the most favorable psychological reactions to pain relative to the other categories: mean total Pain Anxiety Symptoms Scale-20 (PASS-20) score 36.4 (SD 17.9). In contrast, when interference was high on activity, more physical well-being problems were evident e.g. weight: mean BMI 31.0 (SD 7.3) kg/m2, diminished exercise: mean of 1.5 (SD 1.6) exercising sessions per week, and avoidance behavior: mean PASS-20 Escape/Avoidance subscale 3.7 (95% CI: 1.7 to 5.8) scores higher in comparison to activity interference remaining low. With high affective interference, more depressive symptoms: mean BDI-II score 17.7 (SD 7.3), and more cognitive pain anxiety: mean PASS-20 Cognitive Anxiety subscale 2.8 (95% CI 0.7 to 4.8) scores higher in comparison to affective interference remaining low, emerged. Having high interference on both dimensions indicated accumulated risks for reduced physical well-being: mean BMI 29.9 (SD 6.1) kg/m2, mean of 1.2 (SD 1.7) exercising sessions per week, mood problems: mean BDI-II 20.3 (SD 10.6), and negative psychological reactions to pain: mean total PASS-20 score 53.2 (18.4). The results suggest that low interference on both dimensions may allow assessment with only physician consultations, while high interference on either dimension may call attention to distinct issues to be addressed with the help of a physiotherapist or a psychologist, whereas high interference on both dimensions highlights the need for a full multidisciplinary assessment.
慢性疼痛患者进入治疗时具有不同的问题特征,因此需要进行仔细评估,以制定更个体化的治疗计划。在这项横断面研究中,我们根据简明疼痛量表(BPI)的活动和情感疼痛干扰维度的得分,将 320 名进入三级多学科疼痛治疗的患者分为四组。为了确定这种分类系统是否能确定需要进一步评估的问题,我们对三个领域进行了方差分析和多元方差分析:影响身体舒适度的变量(体重指数、运动、物质使用)、心理资源(情绪)和疼痛特定的心理因素(疼痛焦虑、疼痛接受)。结果表明,在两个干扰维度上得分均较低的患者,在体重方面的比较相似:平均体重指数(BMI)为 27.0(SD 6.0)kg/m2,运动方面:每周平均进行 2.4(SD 1.7)次 20 分钟以上的运动,与一般人群相比,平均贝克抑郁指数 II(BDI-II)得分为 11.7(SD 7.5),且相对于其他组,对疼痛的心理反应最有利:平均疼痛焦虑症状量表-20 总得分(PASS-20)为 36.4(SD 17.9)。相比之下,当活动干扰较高时,身体舒适度问题更为明显,例如体重:平均 BMI 为 31.0(SD 7.3)kg/m2,运动减少:每周平均运动次数为 1.5(SD 1.6)次,回避行为:平均 PASS-20 逃避/回避子量表 3.7(95%CI:1.7 至 5.8)分数较高。当情感干扰较高时,抑郁症状更为明显:平均 BDI-II 得分为 17.7(SD 7.3),认知疼痛焦虑更为明显:平均 PASS-20 认知焦虑子量表 2.8(95%CI 0.7 至 4.8)分数较高,而情感干扰较低。两个维度的干扰都较高,表明身体舒适度降低的风险增加:平均 BMI 为 29.9(SD 6.1)kg/m2,每周平均运动次数为 1.2(SD 1.7)次,情绪问题:平均 BDI-II 为 20.3(SD 10.6),对疼痛的负面心理反应:平均 PASS-20 总分为 53.2(18.4)。结果表明,两个维度的干扰均较低,可能只需要医生的咨询评估,而任一维度的干扰较高,可能需要物理治疗师或心理学家的帮助来解决特定问题,而两个维度的干扰均较高,则需要进行全面的多学科评估。