Amphia Ziekenhuis, Department of Neurology, Breda, The Netherlands.
Amsterdam University Medical Centers, University of Amsterdam, Department of Neurology, Amsterdam Neuroscience, The Netherlands.
Clin Infect Dis. 2020 Jun 10;70(12):2469-2475. doi: 10.1093/cid/ciz694.
Performing cranial imaging prior to lumbar punctures (LPs) in patients with suspected central nervous system (CNS) infections has been associated with delayed treatments and poor outcomes. Various guidelines provide different criteria for cranial imaging prior to LP.
We describe the use of cranial imaging in a cohort of adult patients with suspected CNS infections, and evaluated adherence to the recommendations made in the Infectious Disease Society of America (IDSA), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Swedish, and Dutch guidelines. We also analyzed the association between cranial imaging and the time between emergency department entrance and intravenous antibiotic administration.
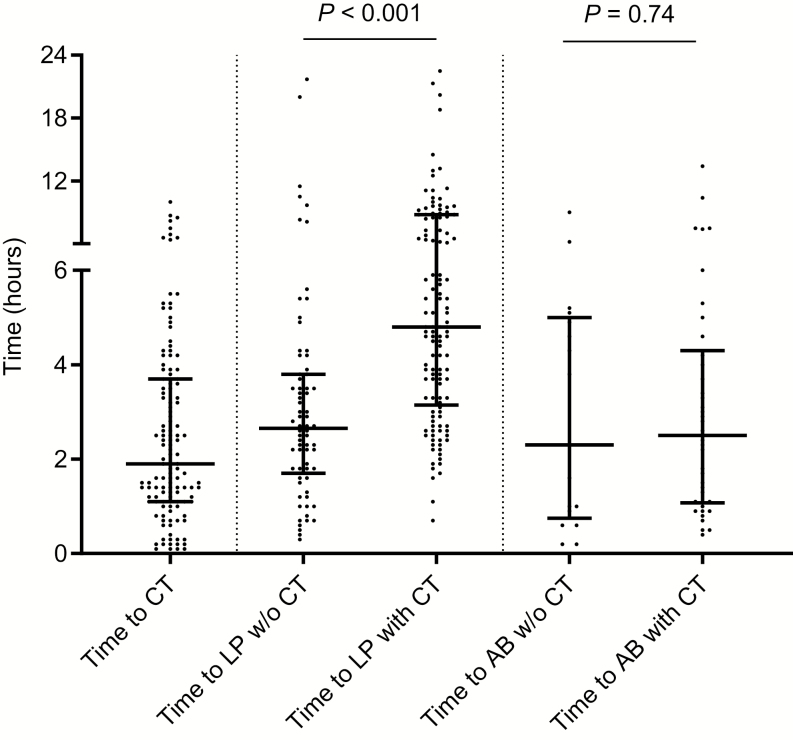
From 2012-2015, 203 patients with suspected CNS infections were included, of whom 56 (27%) were diagnosed with CNS infections and 16 were diagnosed with bacterial meningitis (8%). Cranial imaging, in all cases computed tomography (CT), was performed in 130 patients (64%) and led to the deferral of LPs in 7 (5%). Criteria by the IDSA, ESCMID, Swedish, and Dutch guidelines showed indications for imaging in 64%, 39%, 39%, and 40% of patients, respectively. The times between emergency department arrivals and the start of antibiotic therapy between patients with and without CT before LP were similar (median 134 [interquartile range (IQR) 58-292] vs. 141 minutes [IQR 52-227], respectively; Mann-Whitney U P = .74).
A cranial CT prior to LP was done in the majority of patients with a suspected CNS infection, irrespective of guideline indications. The ESCMID, Swedish, and Dutch guidelines were more restrictive in advising imaging, compared to the IDSA guidelines. Performing cranial imaging prior to LP was not associated with treatment delays in this Dutch cohort study.
在疑似中枢神经系统(CNS)感染的患者中进行颅脑成像检查会导致治疗延迟和预后不良。各种指南为腰椎穿刺(LP)前的颅脑成像提供了不同的标准。
我们描述了在一组疑似 CNS 感染的成年患者中使用颅脑成像的情况,并评估了其对美国传染病学会(IDSA)、欧洲临床微生物学和传染病学会(ESCMID)、瑞典和荷兰指南推荐的遵循情况。我们还分析了颅脑成像与从急诊科进入到静脉使用抗生素之间的时间之间的关联。
2012 年至 2015 年,共纳入 203 例疑似 CNS 感染的患者,其中 56 例(27%)被诊断为 CNS 感染,16 例被诊断为细菌性脑膜炎(8%)。所有患者均行颅脑成像检查(均为计算机断层扫描[CT]),130 例(64%)患者进行了颅脑成像检查,其中 7 例(5%)患者延迟了 LP 检查。IDSA、ESCMID、瑞典和荷兰指南的标准分别显示出 64%、39%、39%和 40%的患者有成像指征。在 LP 前进行 CT 检查的患者和未进行 CT 检查的患者中,从急诊科到达至开始使用抗生素的时间相似(中位数分别为 134 分钟[四分位距(IQR)58-292]和 141 分钟[IQR 52-227];Mann-Whitney U P =.74)。
在疑似 CNS 感染的患者中,大多数患者在 LP 前都进行了颅脑 CT 检查,无论指南的指示如何。与 IDSA 指南相比,ESCMID、瑞典和荷兰指南在建议成像方面更加严格。在这项荷兰队列研究中,LP 前进行颅脑成像与治疗延迟无关。