Usher Institute of Population Health and Informatics, University of Edinburgh, Old Medical School, Teviot Place, Edinburgh EH8 9AG, UK.
Institute of Genetics and Molecular Medicine, University of Edinburgh, Western General Hospital Campus, Crewe Road, Edinburgh, UK.
BMC Med. 2019 Aug 23;17(1):165. doi: 10.1186/s12916-019-1392-8.
The objective of this cross-sectional study was to explore the relationship of detectable C-peptide secretion in type 1 diabetes to clinical features and to the genetic architecture of diabetes.
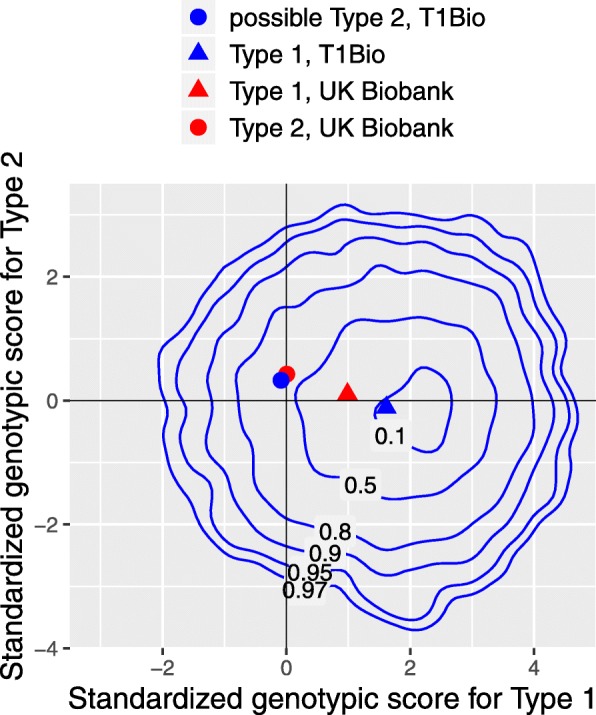
C-peptide was measured in an untimed serum sample in the SDRNT1BIO cohort of 6076 Scottish people with clinically diagnosed type 1 diabetes or latent autoimmune diabetes of adulthood. Risk scores at loci previously associated with type 1 and type 2 diabetes were calculated from publicly available summary statistics.
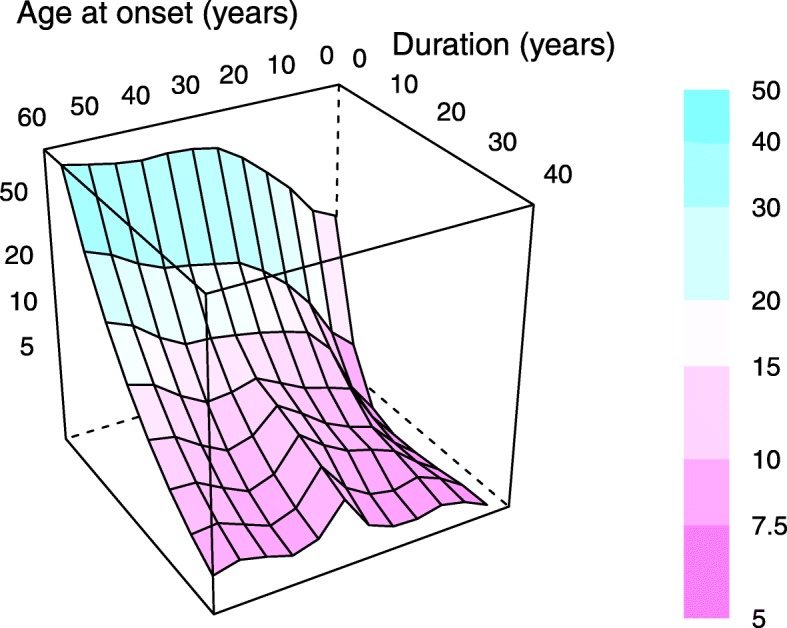
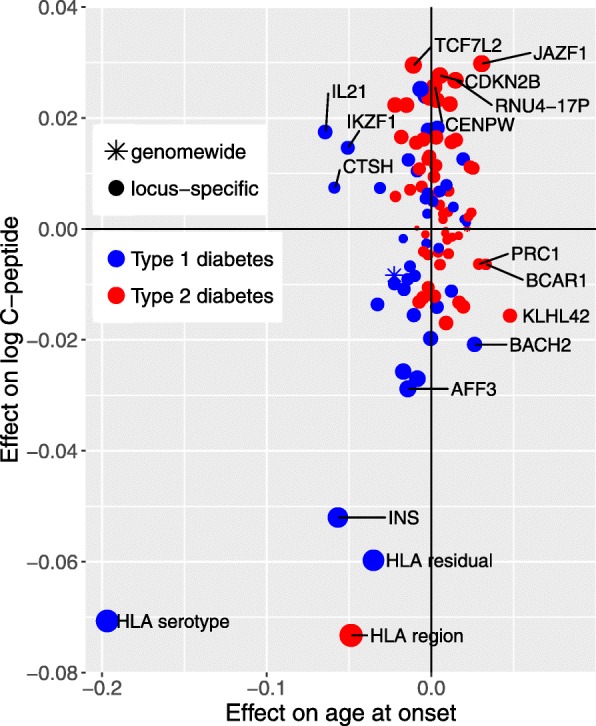
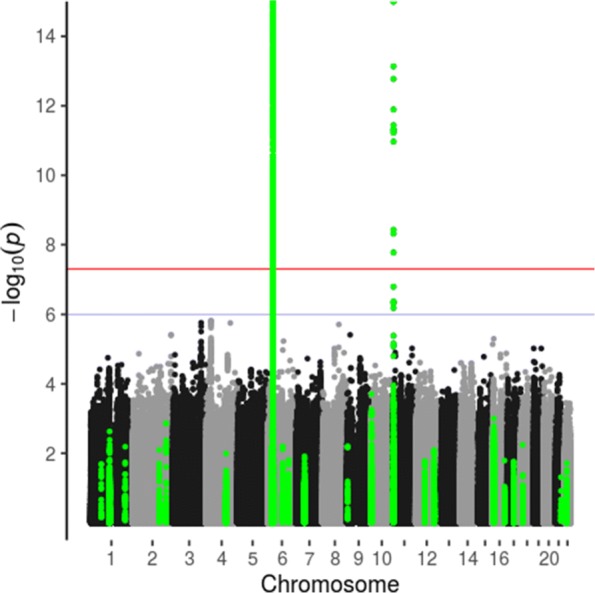
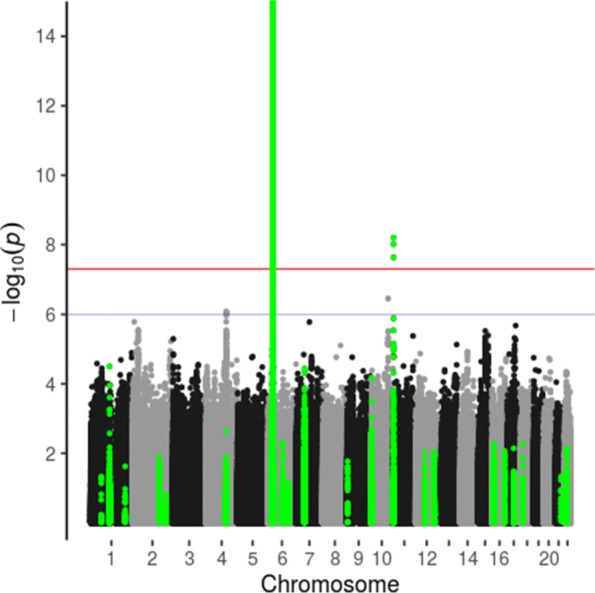
Prevalence of detectable C-peptide varied from 19% in those with onset before age 15 and duration greater than 15 years to 92% in those with onset after age 35 and duration less than 5 years. Twenty-nine percent of variance in C-peptide levels was accounted for by associations with male gender, late age at onset and short duration. The SNP heritability of residual C-peptide secretion adjusted for gender, age at onset and duration was estimated as 26%. Genotypic risk score for type 1 diabetes was inversely associated with detectable C-peptide secretion: the most strongly associated loci were the HLA and INS gene regions. A risk score for type 1 diabetes based on the HLA DR3 and DQ8-DR4 serotypes was strongly associated with early age at onset and inversely associated with C-peptide persistence. For C-peptide but not age at onset, there were strong associations with risk scores for type 1 and type 2 diabetes that were based on SNPs in the HLA region but not accounted for by HLA serotype.
Persistence of C-peptide secretion varies widely in people clinically diagnosed as type 1 diabetes. C-peptide persistence is influenced by variants in the HLA region that are different from those determining risk of early-onset type 1 diabetes. Known risk loci for diabetes account for only a small proportion of the genetic effects on C-peptide persistence.
本横断面研究旨在探讨 1 型糖尿病患者可检测到的 C 肽分泌与临床特征及糖尿病遗传结构的关系。
在苏格兰 SDRNT1BIO 队列中,对 6076 名临床诊断为 1 型糖尿病或成人隐匿性自身免疫性糖尿病的患者进行了非定时血清样本的 C 肽检测。使用公开的汇总统计数据,计算了先前与 1 型和 2 型糖尿病相关的基因座的风险评分。
在起病年龄<15 岁且病程>15 年的患者中,可检测到 C 肽的患病率为 19%,而在起病年龄>35 岁且病程<5 年的患者中,该患病率为 92%。C 肽水平的 29%差异可归因于与男性性别、发病年龄晚和病程短相关的关联。经性别、发病年龄和病程调整后的残余 C 肽分泌 SNP 遗传度估计为 26%。1 型糖尿病的基因型风险评分与可检测到的 C 肽分泌呈负相关:最相关的基因座是 HLA 和 INS 基因区域。基于 HLA DR3 和 DQ8-DR4 血清型的 1 型糖尿病风险评分与发病年龄早呈强烈相关,与 C 肽持续时间呈负相关。与发病年龄相比,C 肽与 HLA 区域中与 1 型和 2 型糖尿病风险评分相关的 SNP 具有很强的关联,但与 HLA 血清型无关。
在临床上被诊断为 1 型糖尿病的患者中,C 肽分泌的持续时间差异很大。C 肽的持续时间受到 HLA 区域中与确定早发性 1 型糖尿病风险不同的变异的影响。糖尿病的已知风险基因座仅占 C 肽持续时间遗传效应的一小部分。