Neyra Javier A, Hu Ming-Chang, Minhajuddin Abu, Nelson Geoffrey E, Ahsan Syed A, Toto Robert D, Jessen Michael E, Moe Orson W, Fox Amanda A
Charles and Jane Pak Center for Mineral Metabolism and Clinical Research, University of Texas Southwestern Medical Center, Dallas, Texas, USA.
Department of Internal Medicine, Division of Nephrology, University of Texas Southwestern Medical Center, Dallas, Texas, USA.
Kidney Int Rep. 2019 May 18;4(8):1131-1142. doi: 10.1016/j.ekir.2019.05.005. eCollection 2019 Aug.
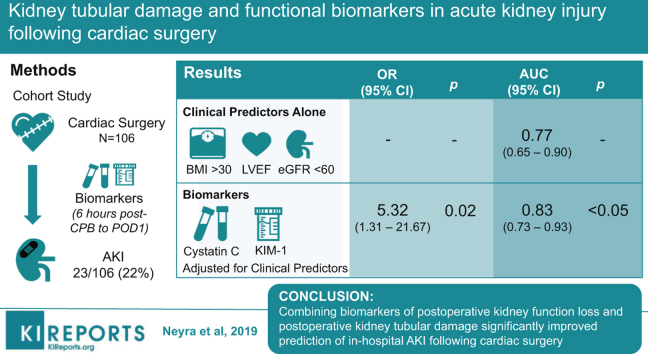
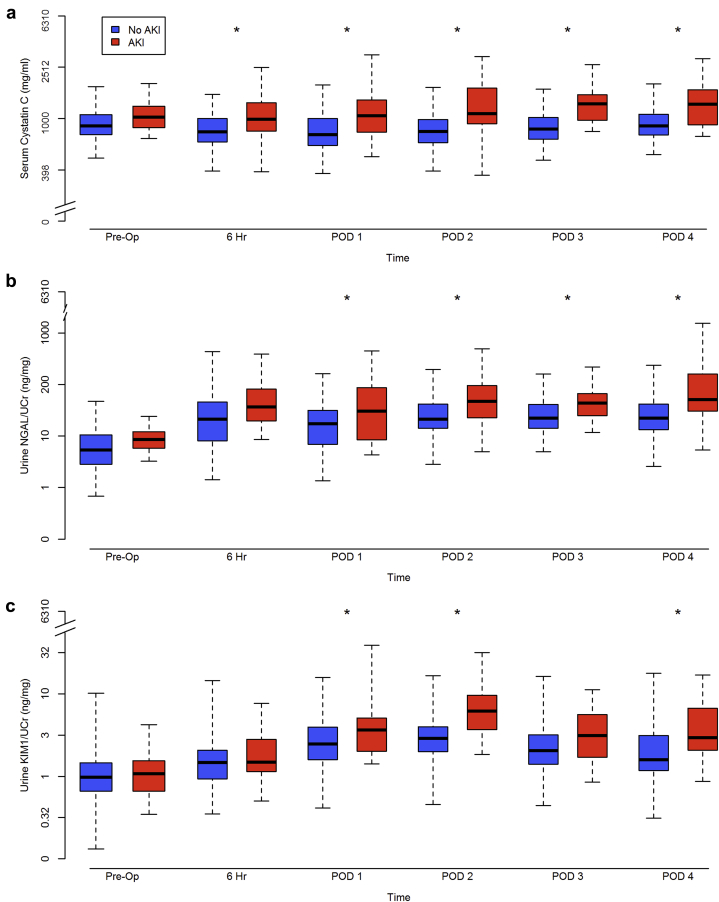
Cardiac surgery-associated acute kidney injury (AKI) is associated with increased morbidity and mortality. We examined the utility of combining biomarkers of kidney function loss (serum cystatin C) and kidney tubular damage (urine neutrophil gelatinase-associated lipocalin [NGAL] and Kidney Injury Molecule-1 [KIM-1]) for the prediction of post-cardiac surgery AKI.
Single-center prospective cohort study of 106 adults undergoing coronary artery bypass grafting and/or valve surgery with cardiopulmonary bypass (CPB). Primary outcome was postoperative in-hospital AKI defined by serum creatinine (SCr)-Kidney Disease: Improving Global Outcomes criteria. Biomarkers were measured preoperatively, 6 hours after CPB and on postoperative days (PODs) 1 to 4.
A total of 23 subjects (21.7%) developed AKI. After adjusting for preoperative left ventricular ejection fraction, body mass index >30 kg/m, and estimated glomerular filtration rate (eGFR) <60 ml/min per 1.73 m, the combination of peak serum cystatin C and peak urine KIM-1/creatinine (Cr) (6 hours post-CPB to POD 1) above optimal cutoff significantly associated with postoperative AKI (odds ratio [OR]: 5.32; 95% confidence interval [CI]: 1.31-21.67; = 0.020). This biomarker combination significantly improved the performance of the clinical model for the prediction of postoperative AKI (area under the curve [AUC]: 0.77, 95% CI: 0.65-0.90 for the clinical model alone versus 0.83, 95% CI: 0.73-0.93 for the clinical model with the addition of biomarker data, = 0.049).
Combining biomarkers of postoperative kidney function loss and postoperative kidney tubular damage significantly improved prediction of in-hospital AKI following cardiac surgery. Future large, multicenter studies are warranted to assess whether panels of biomarkers reflecting distinct pathobiology can be used to guide interventions and improve short- and long-term outcomes in patients undergoing cardiac surgery.
心脏手术相关的急性肾损伤(AKI)与发病率和死亡率增加相关。我们研究了将肾功能丧失生物标志物(血清胱抑素C)和肾小管损伤生物标志物(尿中性粒细胞明胶酶相关脂质运载蛋白[NGAL]和肾损伤分子-1[KIM-1])相结合用于预测心脏手术后AKI的效用。
对106例接受冠状动脉旁路移植术和/或体外循环(CPB)瓣膜手术的成人进行单中心前瞻性队列研究。主要结局是根据血清肌酐(SCr)-《改善全球肾脏病预后》标准定义的术后住院期间AKI。术前、CPB后6小时以及术后第1至4天测量生物标志物。
共有23名受试者(21.7%)发生AKI。在对术前左心室射血分数、体重指数>30 kg/m²以及估计肾小球滤过率(eGFR)<60 ml/min/1.73 m²进行校正后,血清胱抑素C峰值与尿KIM-肌酐(Cr)峰值(CPB后6小时至术后第1天)高于最佳临界值的组合与术后AKI显著相关(比值比[OR]:5.32;95%置信区间[CI]:1.31-21.67;P = 0.020)。这种生物标志物组合显著提高了预测术后AKI的临床模型的性能(曲线下面积[AUC]:仅临床模型为0.77,95%CI:0.65-0.90,添加生物标志物数据后的临床模型为0.83,95%CI:0.73-0.93,P = 0.049)。
将术后肾功能丧失生物标志物和术后肾小管损伤生物标志物相结合可显著改善心脏手术后住院期间AKI的预测。未来有必要进行大型多中心研究,以评估反映不同病理生物学的生物标志物组合是否可用于指导干预并改善心脏手术患者的短期和长期结局。