Quebec Heart & Lung Institute Laval University Quebec City Quebec Canada.
J Am Heart Assoc. 2019 Sep 3;8(17):e013332. doi: 10.1161/JAHA.119.013332. Epub 2019 Aug 23.
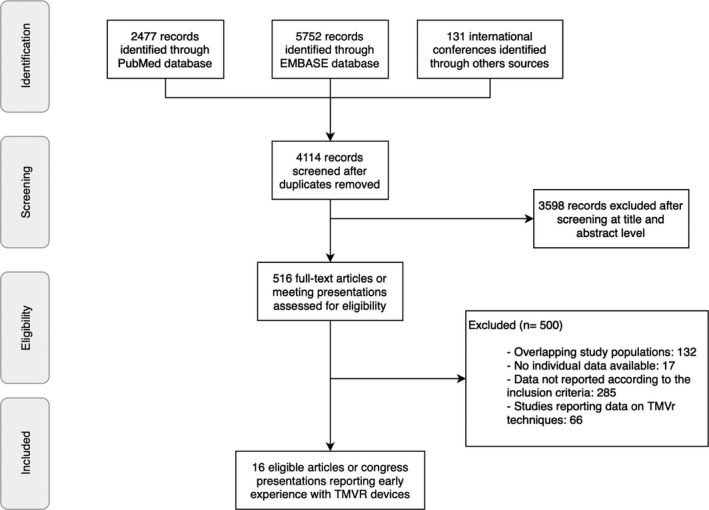
Background Transcatheter mitral valve replacement (TMVR) has emerged as an alternative therapeutic option for the treatment of severe mitral regurgitation in patients with prohibitive or high surgical risk. The aim of this systematic review is to evaluate the clinical procedural characteristics and outcomes associated with the early TMVR experience. Methods and Results Published studies and international conference presentations reporting data on TMVR systems were identified. Only records including clinical characteristics, procedural results, and 30-day and midterm outcomes were analyzed. A total of 16 publications describing 308 patients were analyzed. Most patients (65.9%) were men, with a mean age of 75 years (range: 69-81 years) and Society for Thoracic Surgery Predicted Risk of Mortality score of 7.7% (range: 6.1-8.6%). The etiology of mitral regurgitation was predominantly secondary or mixed (87.1%), and 81.5% of the patients were in New York Heart Association class III or IV. A transapical approach was used in 81.5% of patients, and overall technical success was high (91.7%). Postprocedural mean transmitral gradient was 3.5 mm Hg (range: 3-5.5 mm Hg), and only 4 cases (1.5%) presented residual moderate to severe mitral regurgitation. Procedural and all-cause 30-day mortality were 4.6% and 13.6%, respectively. Left ventricular outflow obstruction and conversion to open heart surgery were reported in 0.3% and 4% of patients, respectively. All-cause and cardiovascular-related mortality rates were 27.6% and 23.3%, respectively, after a mean follow-up of 10 (range: 3 to 24) months. Conclusions TMVR was a feasible, less invasive alternative for treating severe mitral regurgitation in patients with high or prohibitive surgical risk. TMVR was associated with a high rate of successful valve implantation and excellent hemodynamic results. However, periprocedural complications and all-cause mortality were relatively high.
背景 经导管二尖瓣置换术(TMVR)已成为治疗高危或极高手术风险患者严重二尖瓣反流的一种替代治疗选择。本系统评价旨在评估 TMVR 早期经验相关的临床手术特点和结局。
方法和结果 确定了发表的研究和报告 TMVR 系统数据的国际会议演讲。仅分析了包含临床特征、手术结果以及 30 天和中期结局的记录。分析了 16 项描述 308 例患者的研究。大多数患者(65.9%)为男性,平均年龄 75 岁(范围:69-81 岁),胸外科协会预测死亡率为 7.7%(范围:6.1-8.6%)。二尖瓣反流的病因主要为继发性或混合性(87.1%),81.5%的患者为纽约心脏协会心功能分级 III 或 IV 级。经心尖入路在 81.5%的患者中使用,整体技术成功率高(91.7%)。术后平均跨瓣梯度为 3.5mmHg(范围:3-5.5mmHg),仅 4 例(1.5%)存在残余中重度二尖瓣反流。手术和全因 30 天死亡率分别为 4.6%和 13.6%。0.3%和 4%的患者分别报告出现左心室流出道梗阻和中转开胸手术。平均随访 10(范围:3-24)个月后,全因和心血管相关死亡率分别为 27.6%和 23.3%。
结论 TMVR 是一种可行的、微创的替代方法,适用于治疗高危或极高手术风险的严重二尖瓣反流患者。TMVR 与瓣膜植入成功率高和出色的血液动力学结果相关,但围手术期并发症和全因死亡率相对较高。