Aubin Hug, Akhyari Payam, Rellecke Philipp, Pawlitza Christina, Petrov George, Lichtenberg Artur, Kamiya Hiroyuki
Department of Cardiovascular Surgery, University Hospital Düsseldorf, Heinrich-Heine University Düsseldorf, Düsseldorf, Germany.
Department of Cardiac Surgery, Asahikawa Medical University, Asahikawa, Japan.
Front Surg. 2019 Aug 6;6:46. doi: 10.3389/fsurg.2019.00046. eCollection 2019.
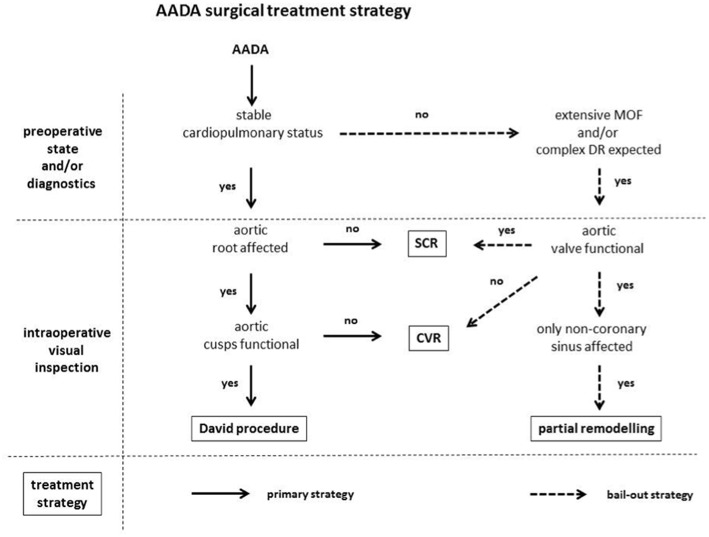
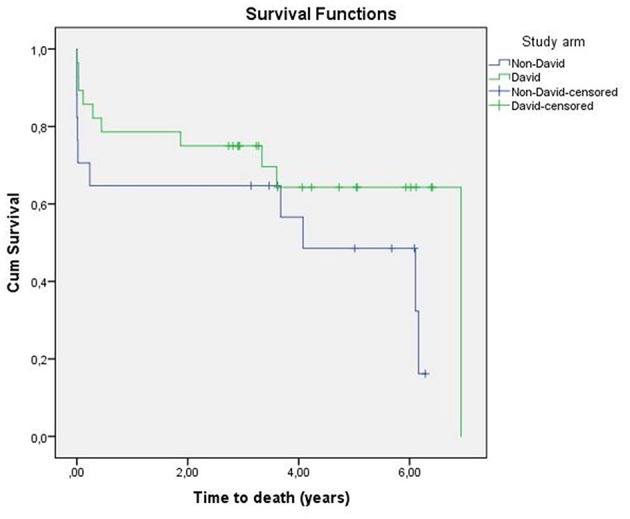
Although, in theory, valve-sparing aortic root replacement () is an ideal surgical option for acute aortic dissection type A (AADA) it is usually not regarded as the first-choice treatment due to the emergency setting and the relative complexity of the procedure. Here, we report the results of a consecutive, single-surgeon series of 45 AADA patients with the as first-choice treatment strategy. Between September 2009 and July 2013 a total of 49 patients with AADA were consecutively operated by the same surgeon at our institution. The was the treatment of choice for the proximal aorta unless aortic valve pathology or critical preoperative patient status advocated against it. Median follow-up was 5.0 years (CI95%, 4.0-6.0). Out of the 45 patients included in this study the was performed in 28 patients (62.2%), while in 17 patients (37.8%) an alternative surgical strategy had to be pursued. Although X-clamping (168.5 ± 41.7 vs. 110.3 ± 51.1 min; = 0.001), cardiopulmonary bypass (CPB) (245.0 ± 62.4 vs. 211.8 ± 123 min; = 0.029) and total operation time (383.8 ± 88.5 vs. 312.8 ± 144.8; = 0.047) were significantly longer in the David-group as compared to the non-David group, there was no difference in major complication rate as well as 30-day (17.9 vs. 23.5%; = 0.645) and 5-year mortality (28.6 vs. 35.3%) between groups. This small series indicates that the may be safe and feasible as a primary surgical treatment strategy for AADA.
尽管理论上保留瓣膜的主动脉根部置换术()对于急性A型主动脉夹层(AADA)是一种理想的手术选择,但由于急诊情况以及该手术相对复杂,它通常不被视为首选治疗方法。在此,我们报告了一组由同一外科医生连续完成的45例AADA患者采用作为首选治疗策略的结果。2009年9月至2013年7月期间,我们机构共有49例AADA患者由同一外科医生连续进行手术。除非存在主动脉瓣病变或术前患者病情危急不适合,否则是近端主动脉的首选治疗方法。中位随访时间为5.0年(CI95%,4.0 - 6.0)。本研究纳入的45例患者中,28例(62.2%)进行了,而17例(37.8%)不得不采用替代手术策略。尽管与非David组相比,David组的交叉阻断时间(168.5±41.7 vs. 110.3±51.1分钟; = 0.001)、体外循环(CPB)时间(245.0±62.4 vs. 211.8±123分钟; = 0.029)和总手术时间(383.8±88.5 vs. 312.8±144.8; = 0.047)明显更长,但两组之间的主要并发症发生率以及30天死亡率(17.9 vs. 23.5%; = 0.645)和5年死亡率(28.6 vs. 35.3%)并无差异。这个小系列研究表明,作为AADA的主要手术治疗策略可能是安全可行的。