Department of Medical Oncology, Leiden University Medical Center, Albinusdreef 2, Leiden, P.O. Box 9600, 2300 RC, Leiden, The Netherlands.
Department of Endocrinology, Leiden University Medical Center, Leiden, The Netherlands.
Breast Cancer Res. 2019 Aug 28;21(1):97. doi: 10.1186/s13058-019-1180-6.
Adjuvant bisphosphonates are associated with improved breast cancer survival in postmenopausal patients. Addition of zoledronic acid (ZA) to neoadjuvant chemotherapy did not improve pathological complete response in the phase III NEOZOTAC trial. Here we report the results of the secondary endpoints, disease-free survival, (DFS) and overall survival (OS).
Patients with HER2-negative, stage II/III breast cancer were randomized to receive the standard 6 cycles of neoadjuvant TAC (docetaxel/doxorubicin/cyclophosphamide) chemotherapy with or without 4 mg intravenous (IV) ZA administered within 24 h of chemotherapy. This was repeated every 21 days for 6 cycles. Cox regression models were used to evaluate the effect of ZA and covariates on DFS and OS. Regression models were used to examine the association between insulin, glucose, insulin growth factor-1 (IGF-1) levels, and IGF-1 receptor (IGF-1R) expression with survival outcomes.
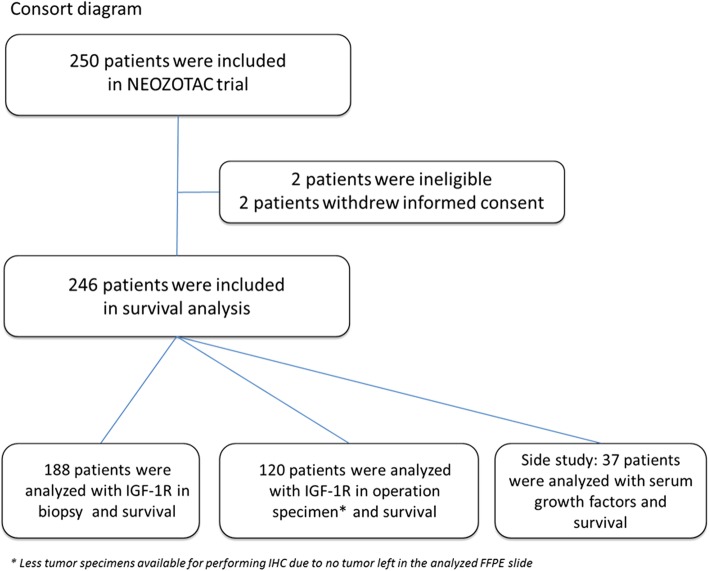
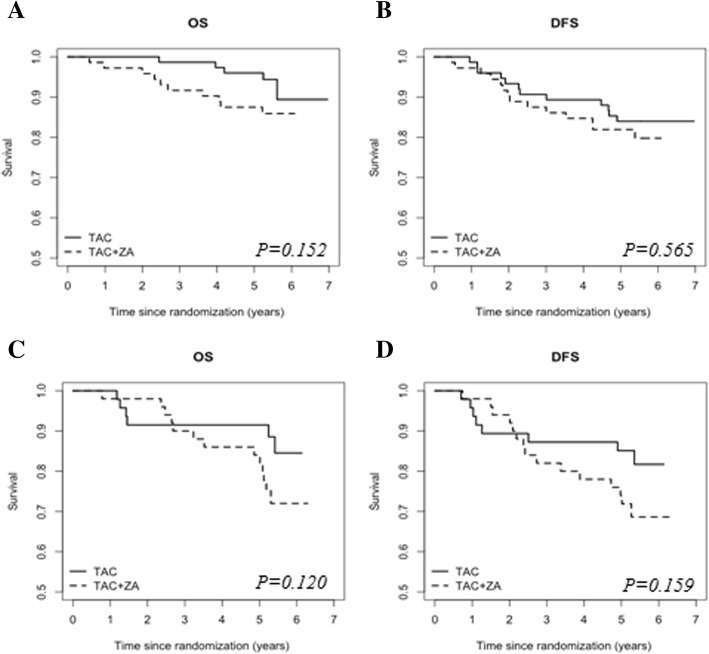
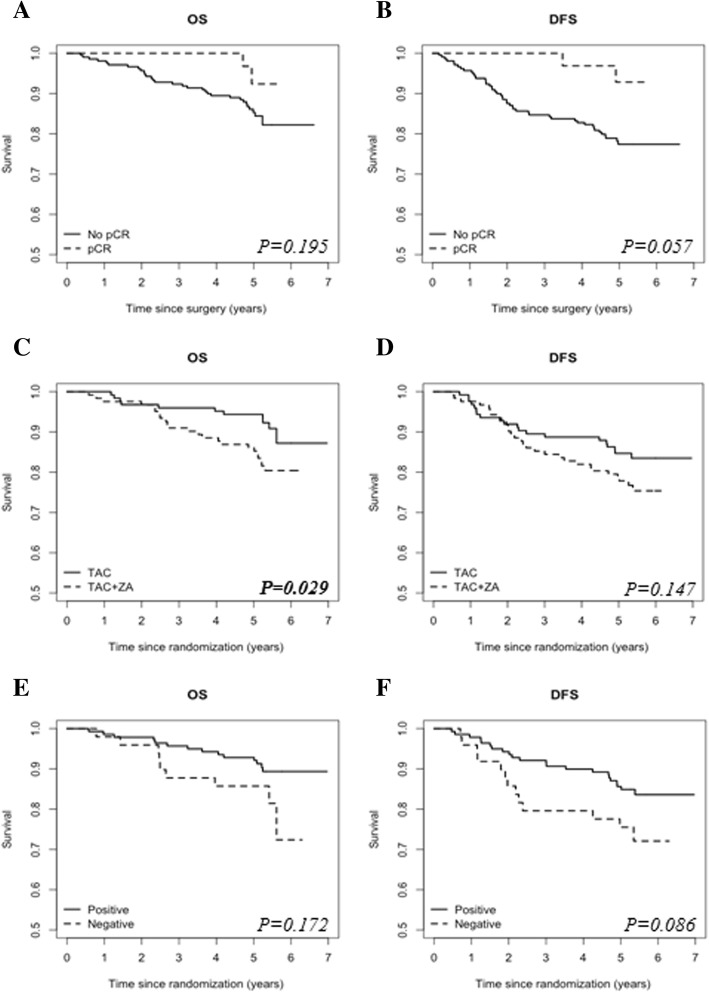
Two hundred forty-six women were eligible for inclusion. After a median follow-up of 6.4 years, OS for all patients was significantly worse for those who received ZA (HR 0.468, 95% CI 0.226-0.967, P = 0.040). DFS was not significantly different between the treatment arms (HR 0.656, 95% CI 0.371-1.160, P = 0.147). In a subgroup analysis of postmenopausal women, no significant difference in DFS or OS was found for those who received ZA compared with the control group (HR 0.464, 95% CI 0.176-1.222, P = 0.120; HR 0.539, 95% CI 0.228-1.273, P = 0.159, respectively). The subgroup analysis of premenopausal patients was not significantly different for DFS and OS ((HR 0.798, 95% CI 0.369-1.725, P = 0.565; HR 0.456, 95% CI 0.156-1.336, P = 0.152, respectively). Baseline IGF-1R expression was not significantly associated with DFS or OS. In a predefined additional study, lower serum levels of insulin were associated with improved DFS (HR 1.025, 95% CI 1.005-1.045, P = 0.014).
Our results suggest that ZA in combination with neoadjuvant chemotherapy was associated with a worse OS in breast cancer (both pre- and postmenopausal patients). However, in a subgroup analysis of postmenopausal patients, ZA treatment was not associated with DFS or OS. Also, DFS was not significantly different between both groups. IGF-1R expression in tumor tissue before and after neoadjuvant treatment did not predict survival.
ClinicalTrials.gov, NCT01099436 , April 2010.
辅助双膦酸盐可改善绝经后患者的乳腺癌生存。在 III 期 NEOZOTAC 试验中,在新辅助化疗中加入唑来膦酸(ZA)并未改善病理完全缓解。在此,我们报告次要终点的结果,无病生存(DFS)和总生存(OS)。
HER2 阴性、II/III 期乳腺癌患者被随机分配接受标准的 6 个周期新辅助 TAC(多西紫杉醇/多柔比星/环磷酰胺)化疗,加或不加 4mg 静脉(IV)ZA,在化疗后 24 小时内给予。这每 21 天重复一次,共 6 个周期。Cox 回归模型用于评估 ZA 和协变量对 DFS 和 OS 的影响。回归模型用于检查胰岛素、葡萄糖、胰岛素生长因子-1(IGF-1)水平和 IGF-1 受体(IGF-1R)表达与生存结果之间的关系。
246 名女性符合纳入标准。中位随访 6.4 年后,所有患者的 OS 明显较差,接受 ZA 治疗的患者(HR 0.468,95%CI 0.226-0.967,P=0.040)。DFS 在治疗组之间无显著差异(HR 0.656,95%CI 0.371-1.160,P=0.147)。在绝经后女性的亚组分析中,与对照组相比,接受 ZA 治疗的患者DFS 或 OS 无显著差异(HR 0.464,95%CI 0.176-1.222,P=0.120;HR 0.539,95%CI 0.228-1.273,P=0.159,分别)。未绝经前患者亚组分析的 DFS 和 OS 无显著差异(HR 0.798,95%CI 0.369-1.725,P=0.565;HR 0.456,95%CI 0.156-1.336,P=0.152,分别)。基线 IGF-1R 表达与 DFS 或 OS 无显著相关性。在一项预先设定的附加研究中,较低的血清胰岛素水平与改善的 DFS 相关(HR 1.025,95%CI 1.005-1.045,P=0.014)。
我们的结果表明,ZA 联合新辅助化疗与乳腺癌患者的 OS 较差相关(绝经前和绝经后患者均如此)。然而,在绝经后患者的亚组分析中,ZA 治疗与 DFS 或 OS 无关。此外,两组之间 DFS 无显著差异。新辅助治疗前后肿瘤组织中 IGF-1R 表达不能预测生存。
ClinicalTrials.gov,NCT01099436,2010 年 4 月。