Karim Sulaiman Sadaf, Pietropaolo Amelia, Skolarikos Andreas, Aboumarzouk Omar, Kallidonis Panagiotis, Tailly Thomas, de Coninck Vincent, Keller Etienne Xavier, Somani Bhaskar Kumar
University Hospital Southampton NHS Trust, Southampton, UK.
2nd Department of Urology, Sismanoglio Hospital, National and Kapodistrian University of Athens, Athens, Greece.
Int Urogynecol J. 2020 Jan;31(1):45-53. doi: 10.1007/s00192-019-04087-5. Epub 2019 Aug 29.
Foreign body (FB) erosion is now recognized as a major long-term complication following previous incontinence surgery. The aim of our systematic review was to ascertain the outcomes of endoscopic management in synthetic sling/mesh erosion following previous gynaecological surgery.
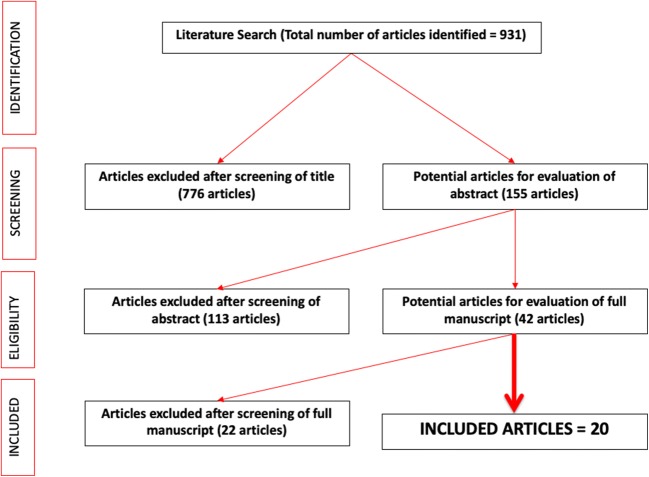
A systematic review in line with PRISMA and Cochrane guidelines was conducted for all English language articles between 1996 and December 2018 for all articles reporting on endoscopic surgical management for eroded FB following previous sling/mesh procedure for incontinence.
Our search produced 931 articles of which 20 articles (198 patients) were included in our review; 149 (75%) had tension-free vaginal tapes (TVT) or tension-free obturator tapes (TOT) as their initial procedure. The site of mesh erosion was the bladder in 134 patients (68%) of which 12 (6%) were in the bladder neck. Urethral mesh erosion was seen in 63 patients (32%) across all studies. The treatment of eroded mesh was by laser and endoscopic excision using an electrode loop or laparoscopic scissors in 108 (55%) and 90 (45%) patients respectively. The initial/final success rate with laser and endoscopic excision was 67%/92% and 80%/98% respectively. The overall complication rates were 24% and 28% in laser and endoscopic groups respectively of which 21% in each group were stress urinary incontinence.
Endoscopic management of FB erosion is an effective minimally invasive technique with good outcomes and minimal morbidity. Management with the use of holmium laser is gaining momentum and could be attempted before open surgical removal. There is a need for comparative data between open surgical excision and endoscopic excision to help better describe the patient's most likely to benefit from the endoscopic technique.
异物侵蚀现已被认为是既往尿失禁手术后的一种主要长期并发症。我们系统评价的目的是确定既往妇科手术后合成吊带/网片侵蚀的内镜治疗结果。
按照PRISMA和Cochrane指南,对1996年至2018年12月间所有报道既往吊带/网片尿失禁手术后侵蚀性异物的内镜手术治疗的英文文章进行系统评价。
我们的检索共得到931篇文章,其中20篇文章(198例患者)纳入我们的评价;149例(75%)最初接受的是无张力阴道吊带术(TVT)或无张力闭孔吊带术(TOT)。134例患者(68%)网片侵蚀部位为膀胱,其中12例(6%)位于膀胱颈。在所有研究中,63例患者(32%)出现尿道网片侵蚀。分别有108例(55%)和90例(45%)患者采用激光和使用电极环或腹腔镜剪刀的内镜切除术治疗侵蚀的网片。激光和内镜切除术的初始/最终成功率分别为67%/92%和80%/98%。激光组和内镜组的总体并发症发生率分别为24%和28%,每组中21%为压力性尿失禁。
内镜治疗异物侵蚀是一种有效的微创技术,效果良好且发病率低。钬激光治疗正逐渐受到关注,可在开放手术切除前尝试。需要开放手术切除与内镜切除之间的比较数据,以更好地描述最可能从内镜技术中获益的患者。