Division of Nephrology, Department of Medicine, Columbia University Medical Center, New York, New York.
The Columbia University Renal Epidemiology (CURE) Group, New York, New York.
JAMA Netw Open. 2019 Aug 2;2(8):e1910312. doi: 10.1001/jamanetworkopen.2019.10312.
In the United States, substantial disparities in access to kidney transplant exist for wait-listed candidates with end-stage renal disease. The implications of transplant centers' willingness to accept kidney offers for access to transplant and mortality outcomes are unknown.
To determine the outcomes for wait-listed kidney transplant candidates after the transplant center's refusal of a deceased donor kidney offer.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study obtained data from the United Network for Organ Sharing Potential Transplant Recipient data set on all deceased donor kidney offers in the United States made between January 1, 2008, and December 31, 2015. The final study cohort included adult patients who were wait-listed for kidney transplant and received at least 1 allograft offer during the study period (N = 280 041). Data analysis was conducted from June 1, 2018, to March 30, 2019.
Candidate state of residence.
Waiting list outcome event groups included received deceased donor allograft, received living donor allograft, died while on the waiting list, removed from the waiting list without a transplant, or still on the waiting list at the end of follow-up.
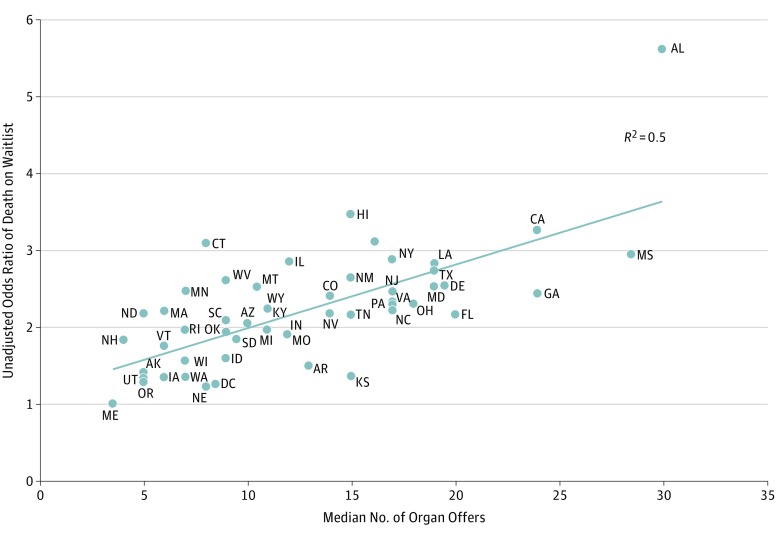
Among the 280 041 kidney transplant candidates included in the study, the mean (SD) age at wait-listing was 51.1 (13.1) years, and male patients were predominant (171 517 [61.2%]). In this cohort, 81 750 candidates (29.2%) received a deceased donor kidney allograft, 30 870 (11.0%) received a living donor allograft, 25 967 (9.3%) died while on the waiting list, and 59 359 (21.2%) were removed from the waiting list. Overall, 10 candidates with at least 1 previous allograft offer died each day during the study period. Time to first offer was similar for candidates who received deceased donor kidney allograft compared with those who died while waiting (median [interquartile range {IQR}] time, 79 [16-426] days vs 78 [17-401] days, respectively). Deceased donor allograft recipients had a median of 17 offers (IQR, 6-44) over 422 days (IQR, 106-909 days), whereas candidates who died while waiting received a median of 16 offers (IQR, 6-41) over 651 days (IQR, 304-1117 days). Most kidneys (84%) were declined on behalf of at least 1 candidate before being accepted for transplant. As reported by centers, organ or donor quality concerns accounted for 8 416 474 (92.6%) of all declined offers, whereas offers were infrequently refused because of patient-related factors (232 193 [2.6%]), logistical limitations (49 492 [0.5%]), or other concerns. The odds of death after an offer and the median number of offers received prior to death varied considerably by state.
This study found that transplant candidates appeared to receive a large number of viable deceased donor kidney offers that were refused on their behalf by transplant centers, potentially exacerbating the detrimental consequences of the organ shortage; increased transparency in organ allocation process and decisions may improve patient-centered care and access to kidney transplant.

在美国,终末期肾病等待移植的患者在获得肾移植方面存在着巨大的差异。移植中心接受肾脏捐赠的意愿对获得移植和死亡率的影响尚不清楚。
确定在移植中心拒绝接受已故供体肾脏供体后,等待移植的肾脏移植候选者的结局。
设计、地点和参与者:本队列研究从美国器官共享联合网络潜在移植受者数据集中获取了 2008 年 1 月 1 日至 2015 年 12 月 31 日期间在美国进行的所有已故供体肾脏供体的所有数据。最终的研究队列包括接受过至少一次移植供体的等待移植的成年患者(N=280041)。数据分析于 2018 年 6 月 1 日至 2019 年 3 月 30 日进行。
候选者的居住州。
等待名单的结局事件组包括接受了已故供体的肾脏移植、接受了活体供体的肾脏移植、在等待名单上死亡、从等待名单上移除但没有进行移植、或在随访结束时仍在等待名单上。
在研究的 280041 名肾脏移植候选者中,等待名单的平均(标准差)年龄为 51.1(13.1)岁,男性患者占主导地位(171517[61.2%])。在这一队列中,81750 名候选者(29.2%)接受了已故供体的肾脏移植,30870 名(11.0%)接受了活体供体的肾脏移植,25967 名(9.3%)在等待名单上死亡,59359 名(21.2%)被从等待名单中移除。总的来说,在研究期间,每天有 10 名至少有一次供体移植的候选者死亡。与等待死亡的候选者相比,接受已故供体肾脏移植的候选者获得首次供体的时间相似(中位数[四分位间距{IQR}],79[16-426]天比 78[17-401]天,分别)。已故供体肾脏受者在 422 天(IQR,106-909 天)中位数有 17 个(IQR,6-44)的供体,而在等待期间死亡的候选者在 651 天(IQR,304-1117 天)中位数有 16 个(IQR,6-41)的供体。在被接受移植之前,大多数(84%)肾脏至少被 1 名候选者拒绝。据中心报告,器官或供体质量问题是所有被拒绝的供体(8416474 个[92.6%])的主要原因,而由于患者相关因素(232193 个[2.6%])、后勤限制(49492 个[0.5%])或其他原因而很少拒绝供体。在收到供体后死亡的可能性以及在死亡前收到的供体数量因州而异。
本研究发现,移植候选者似乎收到了大量的已故供体肾脏供体,这些供体被移植中心代表拒绝,这可能加剧了器官短缺的不利后果;在器官分配过程和决策中增加透明度,可能会改善以患者为中心的护理和获得肾脏移植的机会。