Department of Internal Medicine, School of Medicine, Yale University, New Haven, Connecticut.
Cancer Outcomes, Public Policy, and Effectiveness Research (COPPER) Center, Yale University, New Haven, Connecticut.
Cancer. 2019 Dec 1;125(23):4241-4251. doi: 10.1002/cncr.32439. Epub 2019 Sep 4.
The majority of patients with acute myeloid leukemia (AML) are aged >65 years at the time of diagnosis and are not actively treated. The objective of the current study was to determine the prevalence, temporal trends, and factors associated with no active treatment (NAT) among older patients with AML in the United States.
A retrospective analysis was performed of Surveillance, Epidemiology, and End Results (SEER)-Medicare data from 14,089 patients with AML residing in the United States who were diagnosed with AML at age ≥66 years during 2001 through 2013. NAT was defined as not receiving any chemotherapy, including hypomethylating agents. Multivariable logistic regression models were used to analyze sociodemographic, clinical, and provider characteristics associated with NAT.
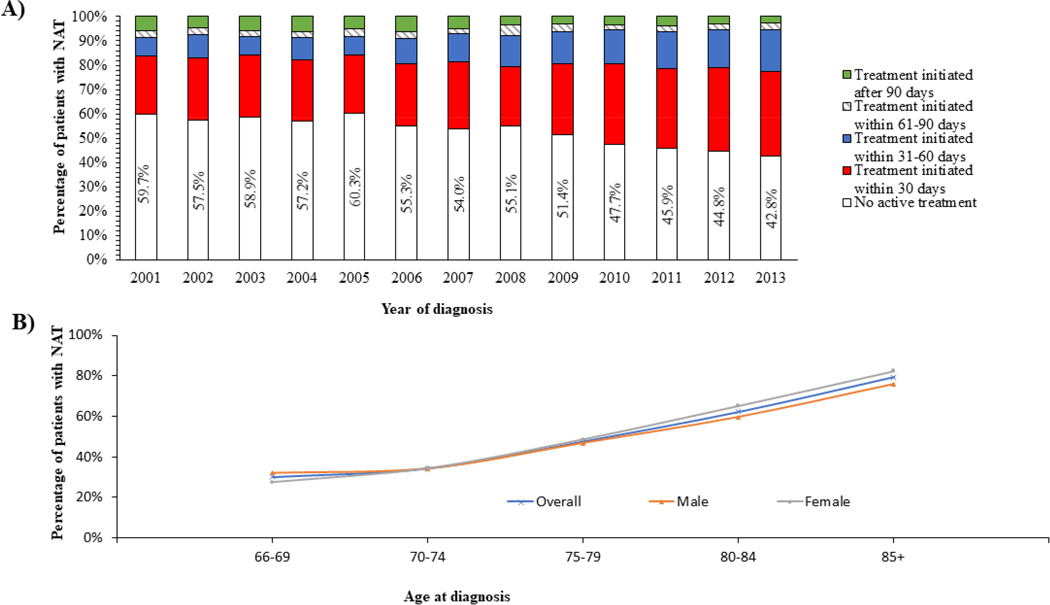
The percentage of patients with NAT decreased over time from 59.7% among patients diagnosed in 2001 to 42.8% among those diagnosed in 2013. The median overall survival for the entire cohort was 82 days from the time of diagnosis. Patients treated with NAT had worse survival compared with those receiving active treatment. Variables found to be associated with higher odds of NAT included older age, certain sociodemographic characteristics (household income within the lowest quartile, residence outside the Northeast region of the United States, and being unmarried), and clinical factors (≥3 comorbidities, the presence of mental disorders, recent hospitalization, and disability).
Greater than one-half of older patients with AML residing in the United States do not receive any active leukemia-directed therapy despite the availability of lower intensity therapies such as hypomethylating agents. Lack of active therapy receipt is associated with inferior survival. Identifying predictors of NAT might improve the quality of care and survival in this patient population, especially as novel therapeutic options with lower toxicity are becoming available.
大多数急性髓细胞白血病(AML)患者在诊断时年龄>65 岁,并未积极治疗。本研究旨在确定美国老年 AML 患者无积极治疗(NAT)的患病率、时间趋势及相关因素。
回顾性分析了 2001 年至 2013 年间在美国居住的年龄≥66 岁的 14089 例 AML 患者的监测、流行病学和最终结果(SEER)-医疗保险数据。NAT 的定义是未接受任何化疗,包括低甲基化剂。采用多变量逻辑回归模型分析与 NAT 相关的社会人口学、临床和提供者特征。
随着时间的推移,接受 NAT 的患者比例从 2001 年诊断的患者的 59.7%下降到 2013 年诊断的患者的 42.8%。整个队列的中位总生存期从诊断时起为 82 天。与接受积极治疗的患者相比,接受 NAT 治疗的患者的生存情况更差。与接受 NAT 的几率较高相关的变量包括年龄较大、某些社会人口学特征(家庭收入处于最低四分位数、居住在美国东北部以外地区、未婚)和临床因素(≥3 种合并症、精神障碍、近期住院和残疾)。
尽管有低强度治疗方法(如低甲基化剂)可用,但居住在美国的老年 AML 患者中有超过一半未接受任何针对白血病的积极治疗。未接受积极治疗与生存质量差相关。确定 NAT 的预测因素可能会改善该患者群体的护理质量和生存,尤其是随着毒性更低的新型治疗选择的出现。