Zhang Guoqing, Wu Bin, Wang Xiaofei, Li Jindong
Department of thoracic surgery, First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan Province, China.
Medicine (Baltimore). 2019 Sep;98(36):e17083. doi: 10.1097/MD.0000000000017083.
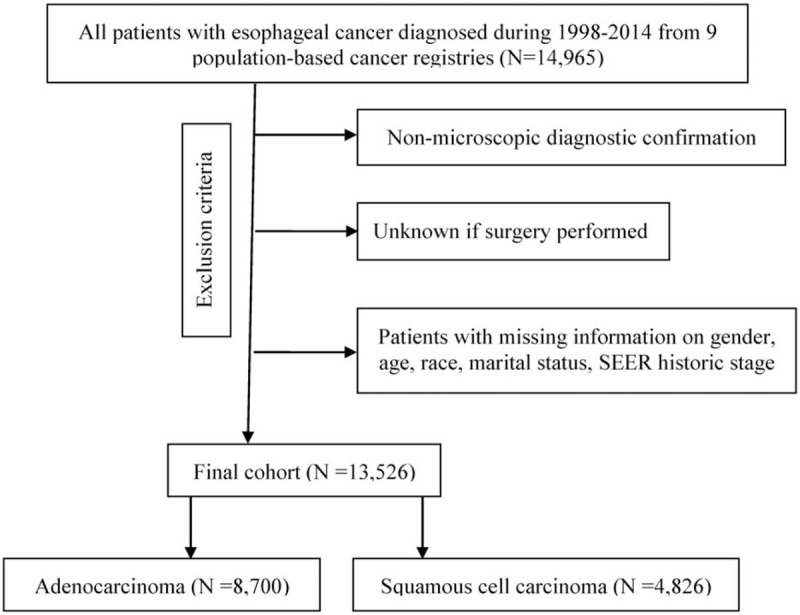
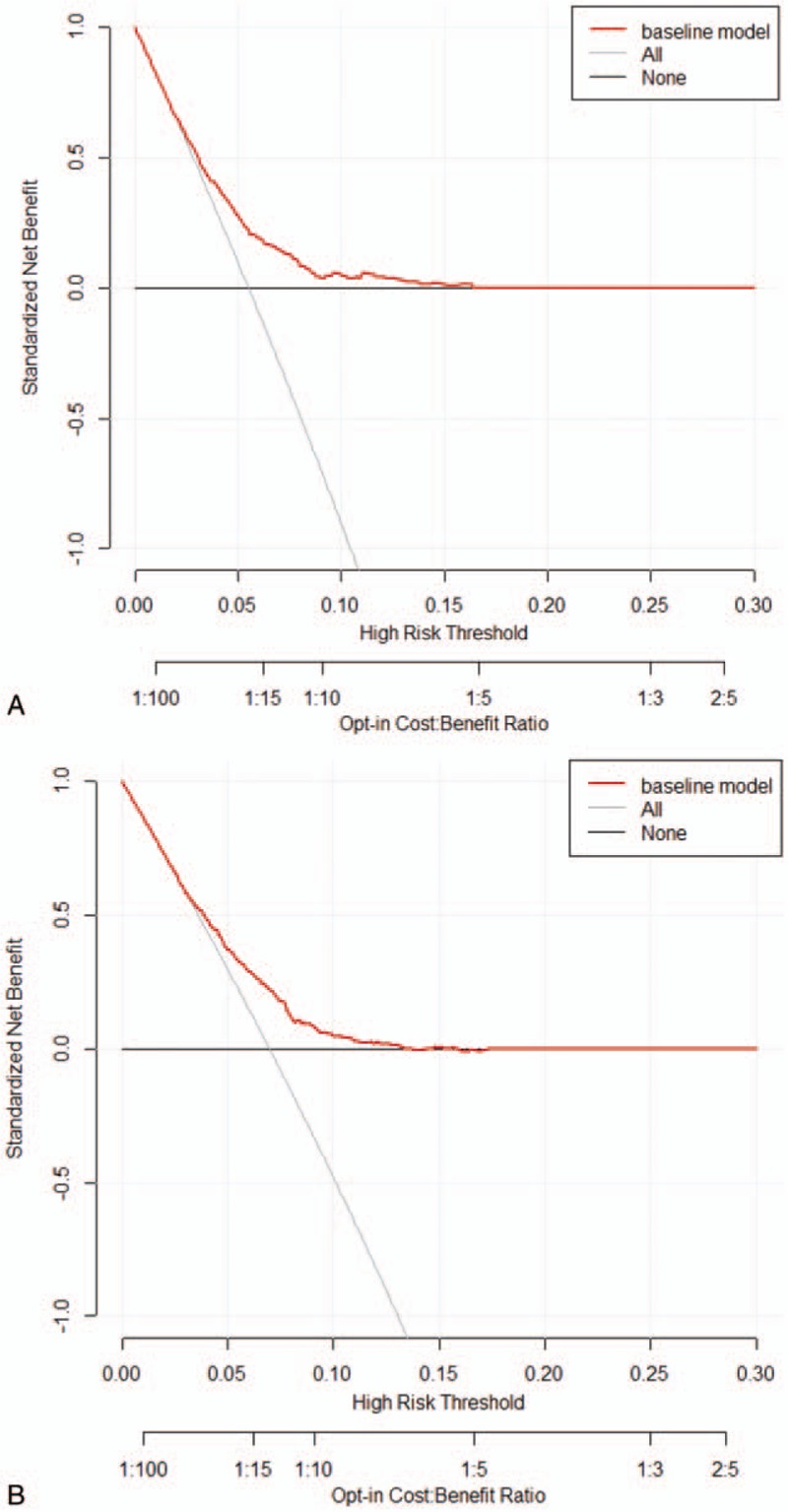
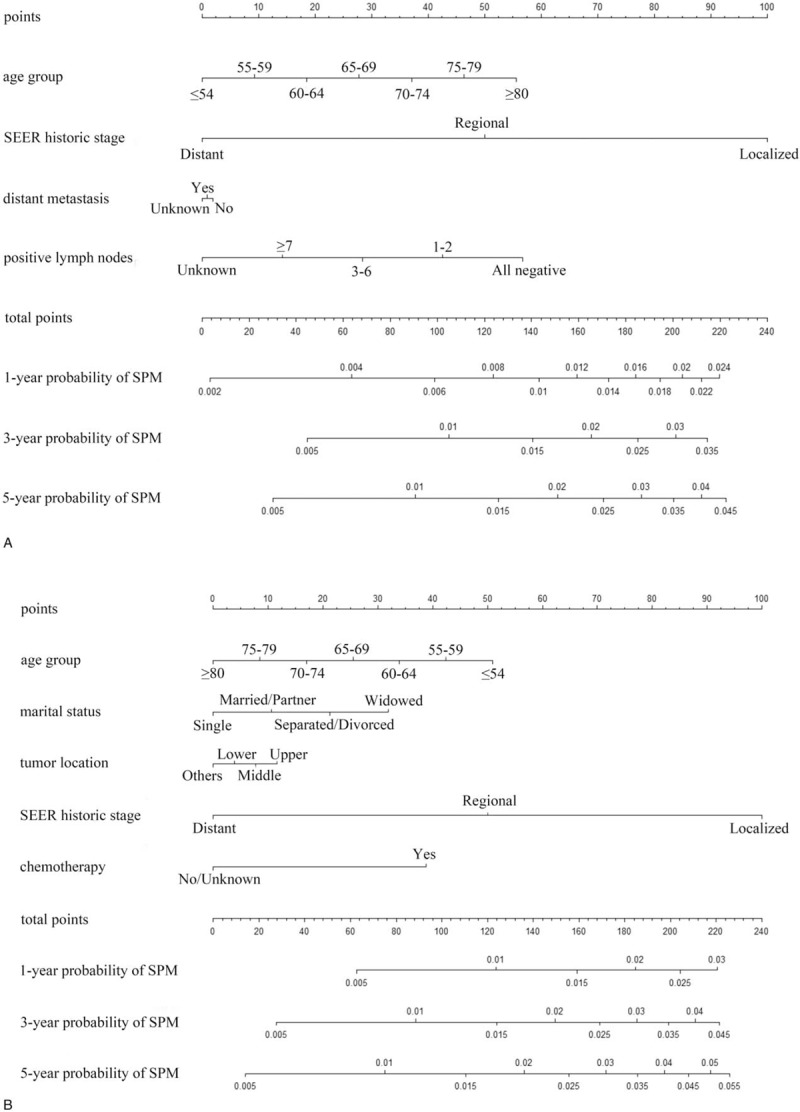
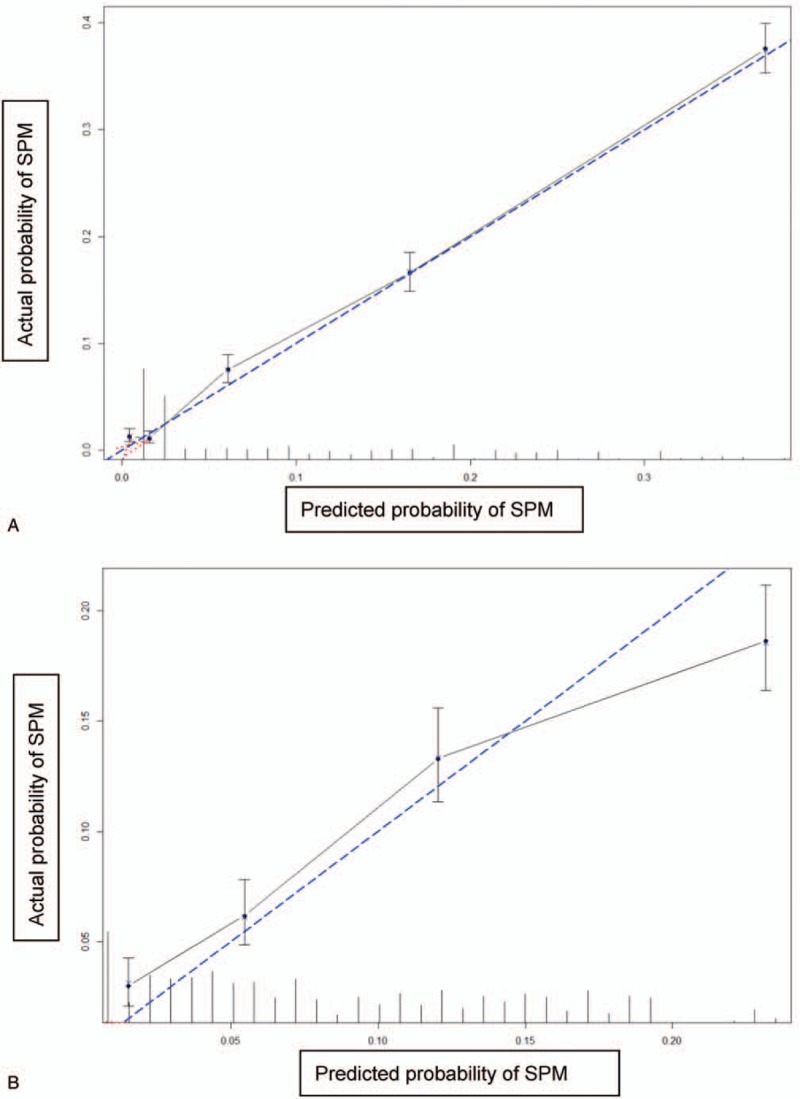
There have been no studies on implementing effective screening models for esophageal adenocarcinoma and squamous cell carcinoma survivors. We used a proportional subdistribution hazards model to estimate second primary malignancy risks among patients with esophageal adenocarcinoma and squamous cell carcinoma. We validated models using a bootstrap cross-validation method and performed decision curve analysis to evaluate their clinical utility. Age group and SEER historic stage were significantly associated with second primary malignancy risk after diagnosis of esophageal adenocarcinoma and squamous cell carcinoma. Saving positive lymph nodes and distant metastasis were significant factors in the adenocarcinoma group, and marital status, tumor location, and chemotherapy were significant factors in the squamous cell carcinoma group. Calibration plots show good concordance between predicted and actual outcomes except in high-probability areas for the risk of a second primary malignancy in patients with esophageal squamous cell carcinoma. Discrimination performances of the Fine-Gray models were evaluated using c-indices, which were 0.691 and 0.662 for second primary malignancies in patients with esophageal adenocarcinoma and squamous cell carcinoma, respectively. Decision curve analysis yielded a range of threshold probabilities (0.020-0.177 and 0.021-0.133 for patients with esophageal adenocarcinoma and squamous cell carcinoma, respectively) at which the clinical net benefit of the risk model was larger than those of hypothetical all-screening and no-screening scenarios. Our nomograms enable selection of patient populations at high risk for a second primary malignancy and thus will facilitate the design of prevention trials for affected populations.
目前尚无关于为食管腺癌和鳞状细胞癌幸存者实施有效筛查模型的研究。我们使用比例子分布风险模型来估计食管腺癌和鳞状细胞癌患者发生第二原发性恶性肿瘤的风险。我们采用自助法交叉验证方法对模型进行验证,并进行决策曲线分析以评估其临床实用性。年龄组和监测、流行病学与最终结果(SEER)历史分期与食管腺癌和鳞状细胞癌诊断后的第二原发性恶性肿瘤风险显著相关。在腺癌组中,阳性淋巴结数量和远处转移是显著因素,而在鳞状细胞癌组中,婚姻状况、肿瘤位置和化疗是显著因素。校准图显示预测结果与实际结果之间具有良好的一致性,但食管鳞状细胞癌患者发生第二原发性恶性肿瘤风险的高概率区域除外。使用c指数评估了Fine-Gray模型的区分性能,食管腺癌和鳞状细胞癌患者发生第二原发性恶性肿瘤的c指数分别为0.691和0.662。决策曲线分析得出了一系列阈值概率(食管腺癌和鳞状细胞癌患者分别为0.020 - 0.177和0.021 - 0.133),在这些阈值概率下,风险模型的临床净效益大于假设的全筛查和不筛查方案。我们的列线图能够选择发生第二原发性恶性肿瘤风险较高的患者群体,从而有助于为受影响人群设计预防试验。