Oncology Pathology, Department of Pathology and Host-Defense, Faculty of Medicine, Kagawa University, Kagawa, Japan.
Department of Pathology, Tokyo Metropolitan Geriatric Hospital, Tokyo, Japan.
PLoS One. 2019 Sep 6;14(9):e0222155. doi: 10.1371/journal.pone.0222155. eCollection 2019.
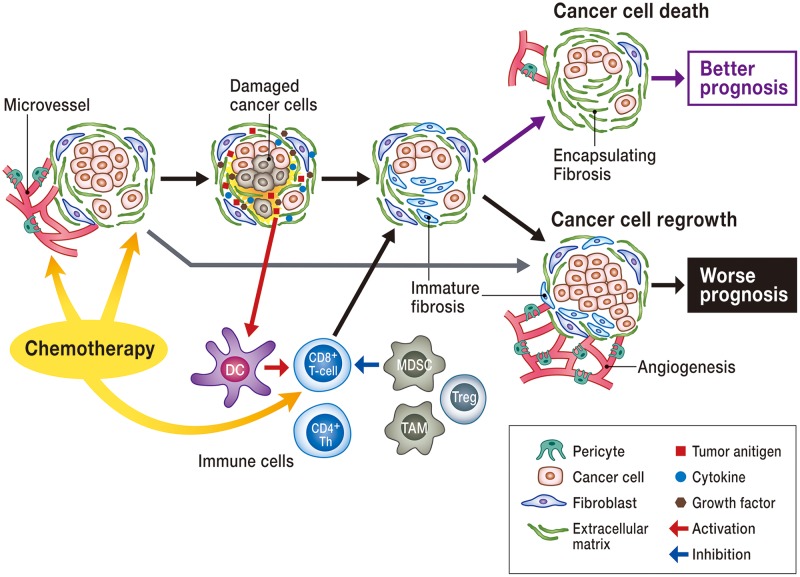
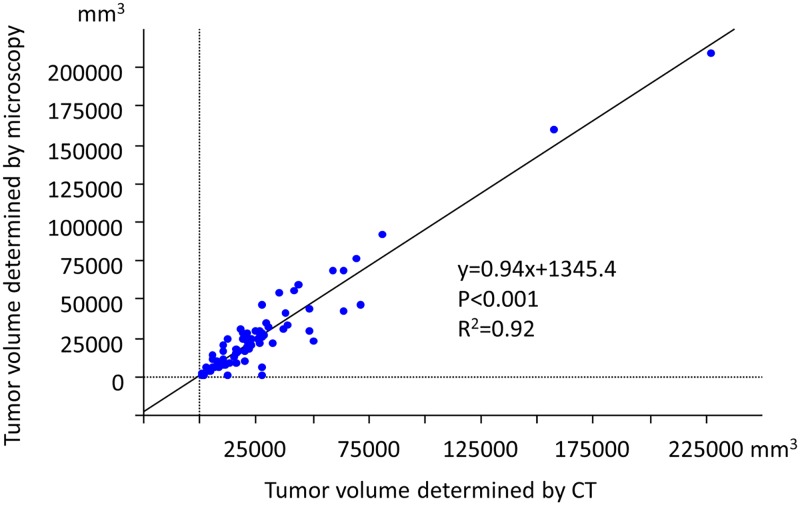
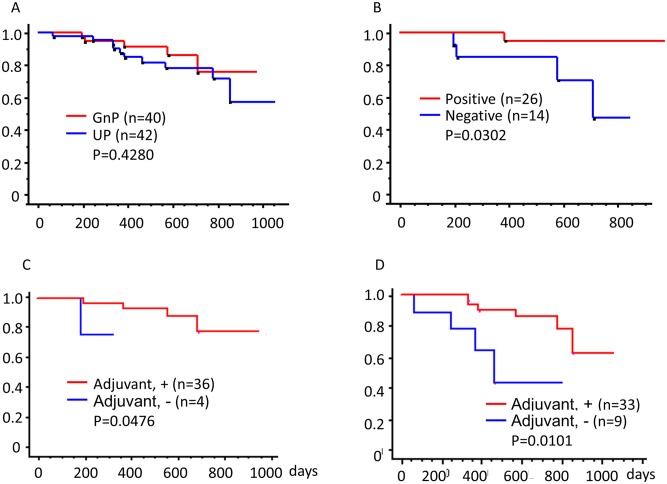
Pathological assessments of the treatment effect are critical for predicting patient outcomes after surgery. This study included 82 localized pancreatic cancer, 40 of whom were treated with neoadjuvant therapy (NAT) using four courses of gemcitabine plus nab-paclitaxel (GnP) followed by pancreatectomy (GnP group). The remaining 42 patients were treated with upfront pancreatectomy (UP) followed by adjuvant chemotherapy (UP group). We reviewed clinicopathological data of these patients to assess differences between the GnP and UP groups and further evaluate the prognostic impact of residual tumors after GnP treatment. Adjuvant treatment (S1, GnP or gemcitabine) was administered for 36 patients in the GnP group and 33 patients in the UP group. Compared to the UP group, the GnP group showed lower serum CA19-9 levels, microscopic tumor volume, and tumor-stroma ratio and decreased number of lymph node metastasis and vascular invasion. Higher incidence of encapsulating fibrosis was observed in the GnP group than in the UP group. Relative to the UP group (69%), a higher R0 rate was observed in the GnP group (85%). As for prognosis, encapsulating fibrosis was correlated with the overall survival of patients in the GnP group. However, overall survival did not show any correlation with other clinicopathological factors, including tumor reduction ratio (determined by computed tomography) and tumor regression grade (determined following criteria of Evans' grading system or those of the College of American Pathologists). In conclusion, the present study revealed that GnP-induced encapsulating fibrosis could predict patients' outcome. Nevertheless, large cohort studies are warranted to further evaluate the prognostic value of fibrosis, possibly with the help of imaging and biomarkers.
术后病理评估对于预测患者的治疗效果至关重要。本研究纳入了 82 例局限性胰腺癌患者,其中 40 例接受了新辅助治疗(NAT),采用吉西他滨加 nab-紫杉醇(GnP)联合治疗 4 个疗程,然后行胰切除术(GnP 组)。其余 42 例患者接受了胰切除术(UP),随后接受辅助化疗(UP 组)。我们回顾了这些患者的临床病理数据,以评估 GnP 组和 UP 组之间的差异,并进一步评估 GnP 治疗后残留肿瘤的预后影响。GnP 组 36 例和 UP 组 33 例患者接受了辅助治疗(S1、GnP 或吉西他滨)。与 UP 组相比,GnP 组患者的血清 CA19-9 水平、肿瘤体积、肿瘤间质比以及淋巴结转移和血管侵犯的数量均较低。GnP 组包膜纤维化的发生率高于 UP 组。与 UP 组(69%)相比,GnP 组的 R0 率更高(85%)。就预后而言,GnP 组包膜纤维化与患者的总生存率相关。然而,总体生存与包括肿瘤缩小率(通过计算机断层扫描确定)和肿瘤消退分级(根据 Evans 分级系统或美国病理学家学院标准确定)在内的其他临床病理因素均无相关性。总之,本研究表明 GnP 诱导的包膜纤维化可预测患者的预后。然而,需要进行更大规模的队列研究来进一步评估纤维化的预后价值,可能需要借助影像学和生物标志物。