Department of Internal Medicine, Yonsei University, Wonju College of Medicine, Wonju, Republic of Korea.
Department of Internal Medicine, Yonsei University, Wonju College of Medicine, Wonju, Republic of Korea
Heart. 2020 Feb;106(4):292-298. doi: 10.1136/heartjnl-2019-315240. Epub 2019 Sep 6.
This study evaluated the relationship between guideline adherence for recommended therapy on discharge and relevant 60-day and 1-year clinical outcomes in patients with acute heart failure (HF) with reduced ejection fraction and atrial fibrillation (AF).
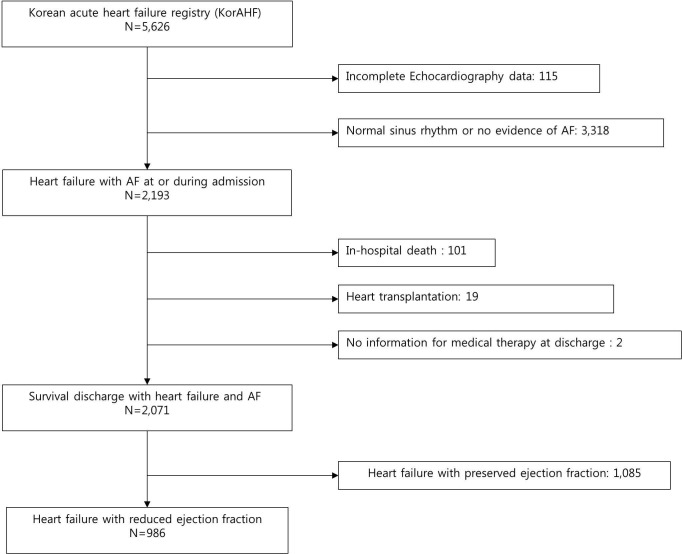
Of 5625 acute patients with HF in the Korean Acute Heart Failure registry, 986 patients with HF and documented AF were analysed. Guideline adherence scores were calculated for the prescription of ACE inhibitors, angiotensin receptor blockers, β-blockers, mineralocorticoid receptor antagonists and anticoagulants.
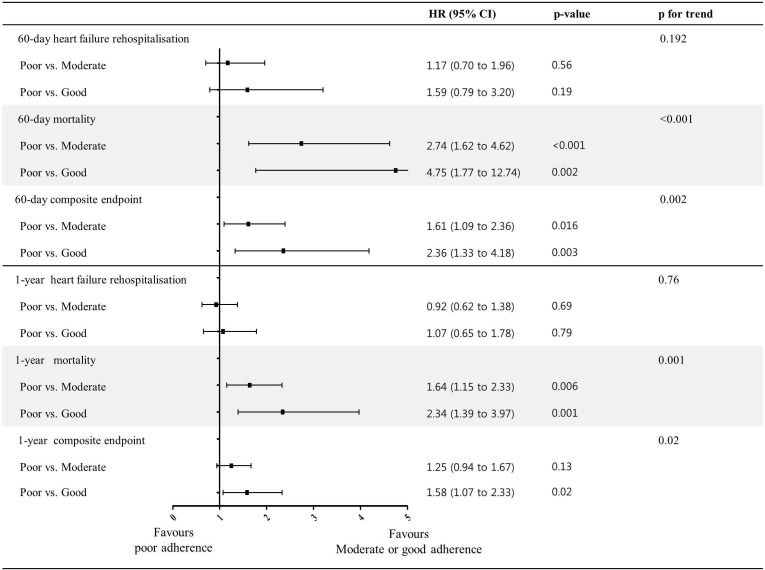
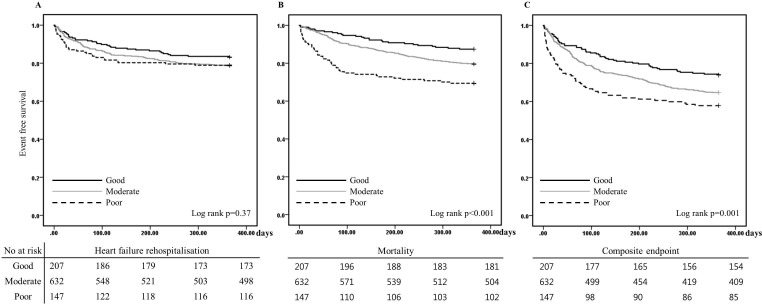
In patients with HF with AF, there was a significant trend of reduced 60-day and 1-year mortality rates and the composite end point with guideline adherence. According to the Cox proportion hazard model, poor adherence was associated with a significantly higher risk of 60-day mortality (HR 4.75; 95% CI 1.77 to 12.74) and the composite end point (HR 2.36; 95% CI 1.33 to 4.18) compared with good adherence. Furthermore, poor adherence was associated with a significantly higher risk of 1-year mortality compared with moderate (HR 1.64; 95% CI 1.15 to 2.33) and good adherence (HR 2.34; 95% CI 1.39 to 3.97) and with a higher risk of the 1-year composite end point compared with good adherence (HR 1.58; 95% CI 1.07 to 2.33).
Better adherence to guidelines was associated with better 60-day and 1-year prognoses in patients with HF with AF.
本研究评估了推荐疗法出院时的指南遵循与射血分数降低的急性心力衰竭(HF)合并心房颤动(AF)患者相关的 60 天和 1 年临床结局之间的关系。
在韩国急性心力衰竭注册中心的 5625 例急性 HF 患者中,分析了 986 例 HF 合并有记录的 AF 患者。根据 ACEI、血管紧张素受体阻滞剂、β受体阻滞剂、盐皮质激素受体拮抗剂和抗凝剂的处方,计算指南遵循评分。
在合并 AF 的 HF 患者中,随着指南遵循程度的提高,60 天和 1 年死亡率和复合终点呈显著降低趋势。根据 Cox 比例风险模型,与良好遵循相比,较差的遵循与 60 天死亡率(HR 4.75;95%CI 1.77 至 12.74)和复合终点(HR 2.36;95%CI 1.33 至 4.18)的风险显著更高。此外,与中度(HR 1.64;95%CI 1.15 至 2.33)和良好(HR 2.34;95%CI 1.39 至 3.97)相比,较差的遵循与 1 年死亡率的风险显著更高,与良好的遵循相比,与 1 年复合终点的风险更高(HR 1.58;95%CI 1.07 至 2.33)。
更好地遵循指南与 HF 合并 AF 患者的 60 天和 1 年预后更好相关。