Department of Neurosurgery and Neuro-Oncology, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-Sen University Cancer Center, 651 Dongfeng Road East, Guangzhou, 510060, China.
Department of Traditional Chinese Medicine, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, China.
J Neurooncol. 2019 Oct;145(1):125-134. doi: 10.1007/s11060-019-03278-w. Epub 2019 Sep 6.
We aim to investigate the impacts of extent of resection and adjuvant radiotherapy on survival of high-grade meningiomas (WHO grade II-III) according to modern diagnosis and management.
Patients with high-grade meningiomas were identified in the Surveillance Epidemiology and End Results (SEER) database between 2000 and 2015 and used for survival analysis. Propensity score matching (PSM) was conducted to reduce selection bias. Another 92 patients from Sun Yat-sen University Cancer Center (SYSUCC) were used for validation.
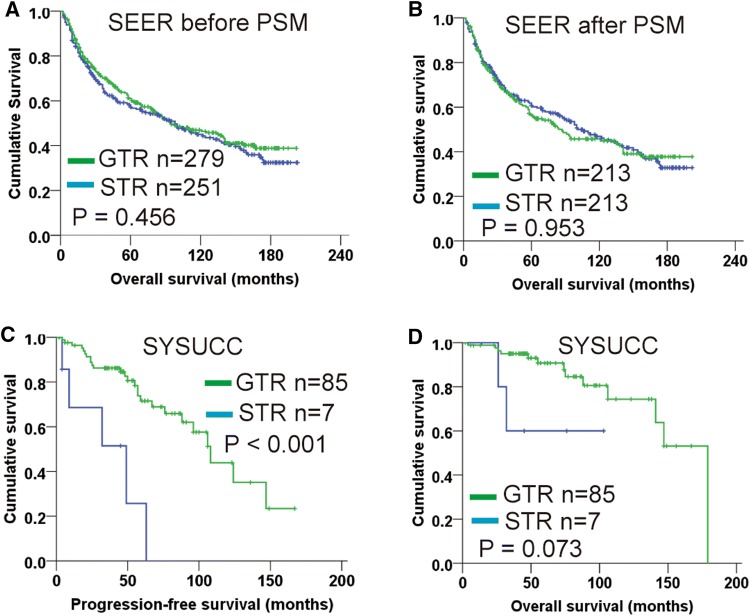
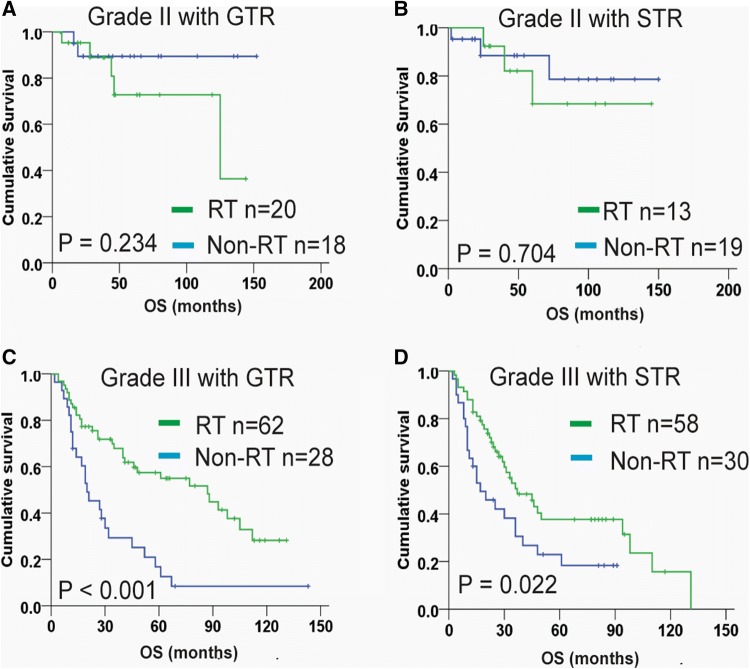
530 patients were enrolled from SEER. Patients with gross total resection (GTR) had no significantly different overall survival (OS) compared with those with subtotal resection (STR), even after performing PSM between these two groups. Multivariable analysis found that age ≥ 65 years (HR 2.22, P < 0.001), tumor diameter > 6 cm (HR 1.59, P = 0.004) and grade III tumor (HR 4.31, P < 0.001) were associated with worse OS. Stratification analysis showed that adjuvant radiotherapy conferred significantly improved OS for grade III meningiomas, but not for grade II meningiomas, regardless of resection extent. In SYSUCC cohort, resection extent was also not significantly associated with OS. However, patients with GTR (Simpson grade I-III) had distinctly increased progression-free survival (PFS) than those with STR (P < 0.001). Additionally, for grade II meningiomas after GTR, radiotherapy was unable to improve OS and PFS.
On modern management of high-grade meningiomas, GTR does not improve OS, but seems to be associated with increased PFS. Radiotherapy is reasonable as a supplement for treating grade III meningiomas, whereas its effect for grade II meningiomas remains uncertain and needs further validation by prospective study.
本研究旨在探讨在现代诊断和治疗水平下,最大限度切除术和辅助放疗对高级别脑膜瘤(WHO 分级 II-III 级)患者生存的影响。
本研究通过监测、流行病学和最终结果(SEER)数据库,纳入了 2000 年至 2015 年间诊断为高级别脑膜瘤的患者,并进行生存分析。采用倾向评分匹配(PSM)以减少选择偏倚。同时,本研究还纳入了中山大学肿瘤防治中心(SYSUCC)的 92 例患者进行验证。
SEER 数据库共纳入 530 例患者。尽管对这两组患者进行了 PSM,但全切组(GTR)患者的总生存期(OS)与次全切组(STR)患者相比并无显著差异。多变量分析发现,年龄≥65 岁(HR 2.22,P<0.001)、肿瘤直径>6cm(HR 1.59,P=0.004)和 III 级肿瘤(HR 4.31,P<0.001)与 OS 较差相关。分层分析显示,辅助放疗显著改善了 III 级脑膜瘤患者的 OS,但对 II 级脑膜瘤患者则无显著影响,无论切除程度如何。在 SYSUCC 队列中,切除程度也与 OS 无显著相关性。然而,GTR 组(Simpson 分级 I-III)的无进展生存期(PFS)明显长于 STR 组(P<0.001)。此外,对于 GTR 后的 II 级脑膜瘤,放疗并不能改善 OS 和 PFS。
在现代高级别脑膜瘤的治疗中,GTR 并不能提高 OS,但似乎与 PFS 的增加有关。放疗对于治疗 III 级脑膜瘤是合理的选择,而对于 II 级脑膜瘤的疗效仍不确定,需要进一步通过前瞻性研究进行验证。