Anne Bates Leach Eye Center, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, Florida, USA; Ophthalmic Biophysics Center, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, Florida, USA; Florida Lions Ocular Pathology Laboratory, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, Florida, USA.
Ophthalmic Biophysics Center, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, Florida, USA.
Am J Ophthalmol. 2019 Dec;208:387-396. doi: 10.1016/j.ajo.2019.08.027. Epub 2019 Sep 5.
To report clinical outcomes of rose bengal photodynamic antimicrobial therapy (RB-PDAT) as an adjunct treatment for severe, progressive infectious keratitis.
Consecutive interventional case series.
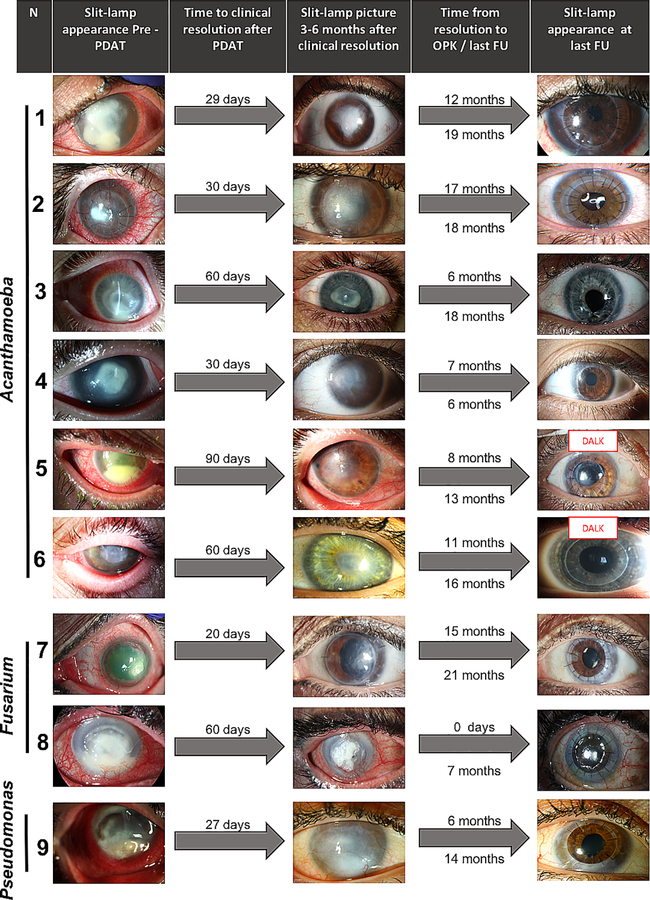
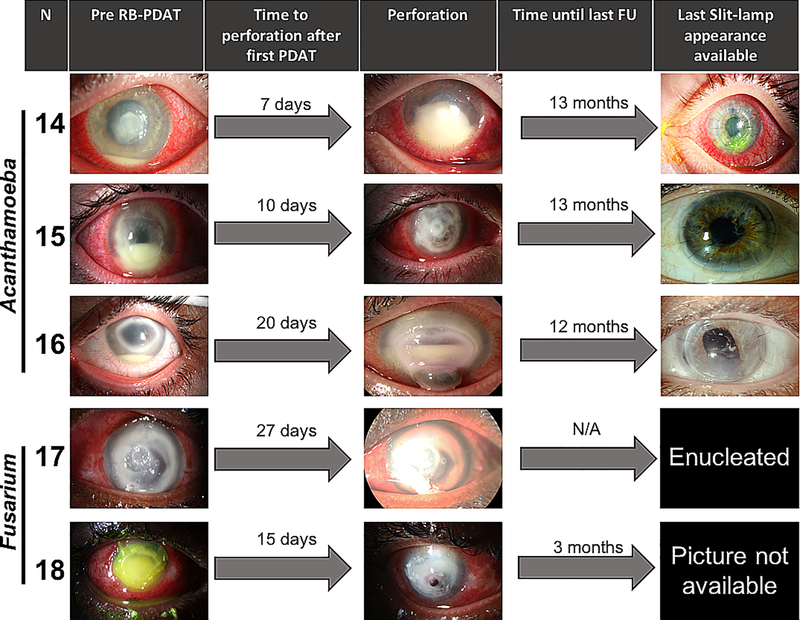
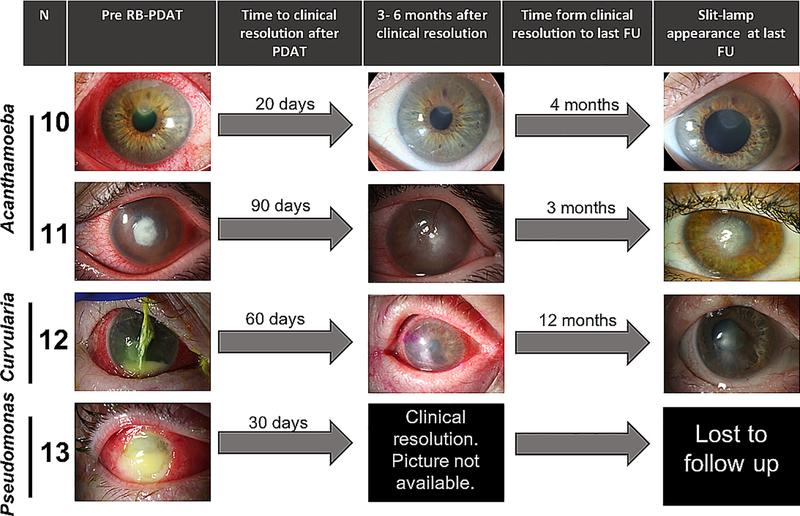
Patients with progressive infectious keratitis unresponsive to standard medical therapy underwent RB-PDAT at the Bascom Palmer Eye Institute from January 2016 through March 2018. RB-PDAT was performed by applying a solution of rose bengal (0.1% or 0.2% RB in balanced salt solution) to the de-epithelialized cornea for 30 minutes, followed by irradiation with a 6 mW/cm custom-made green LED source for 15 minutes (5.4 J/cm).
The current study included 18 patients (7 male and 11 female) ranging from 17 to 83 years old. Acanthamoeba was the most frequent microbe (10/17; 59%), followed by Fusarium spp. (4/17; 24%), Pseudomonas aeruginosa (2/17; 12%), and Curvularia spp. (1/17; 6%); 1 patient had no confirmed microbiologic diagnosis. Main clinical risk factor for keratitis included contact lens wear (79%). The average area of epithelial defect prior to first RB-PDAT was 32 ± 27 mm and average stromal depth hyperreflectivity measured with anterior segment optical coherence tomography was 269 ± 75 μm. Successful RB-PDAT (avoidance of therapeutic keratoplasty) was achieved in 72% of the cases, with an average time to clinical resolution (decreased pain and inflammation with re-epithelialization and infiltrate resolution) of 46.9 ± 26.4 days after RB-PDAT. Time of follow-up after RB-PDAT was 13.3 ± 5.7 months.
RB-PDAT can be considered as an adjunct therapy for cases of severe, progressive infectious keratitis before performing a therapeutic keratoplasty.
报告孟加拉玫瑰红光动力抗菌疗法(RB-PDAT)作为严重、进行性感染性角膜炎辅助治疗的临床结果。
连续的干预性病例系列研究。
2016 年 1 月至 2018 年 3 月,在巴斯科姆·帕尔默眼科研究所,对经标准药物治疗无效的进行性感染性角膜炎患者进行 RB-PDAT。RB-PDAT 通过将孟加拉玫瑰红(0.1%或 0.2% RB 在平衡盐溶液中)溶液应用于去上皮化角膜 30 分钟,然后用定制的 6 mW/cm 绿光 LED 源照射 15 分钟(5.4 J/cm)来完成。
本研究纳入了 18 名患者(7 名男性和 11 名女性),年龄 17 至 83 岁。棘阿米巴是最常见的微生物(17 例中的 10 例;59%),其次是镰刀菌属(17 例中的 4 例;24%)、铜绿假单胞菌(17 例中的 2 例;12%)和弯孢属(17 例中的 1 例;6%);1 例患者无明确的微生物学诊断。角膜炎的主要临床危险因素是角膜接触镜佩戴(79%)。第一次 RB-PDAT 前上皮缺损的平均面积为 32 ± 27mm,前节光学相干断层扫描测量的平均基质深度高反射性为 269 ± 75μm。72%的病例成功进行了 RB-PDAT(避免了治疗性角膜移植),平均临床缓解时间(疼痛减轻、炎症消退,上皮再形成和浸润消退)为 RB-PDAT 后 46.9 ± 26.4 天。RB-PDAT 后的随访时间为 13.3 ± 5.7 个月。
在进行治疗性角膜移植之前,RB-PDAT 可作为严重、进行性感染性角膜炎的辅助治疗。