Department of Radiology, the First Affiliated Hospital of Chongqing Medical University, 1 Youyi Road, Yuzhong District, Chongqing, 400016, China.
BMC Musculoskelet Disord. 2019 Sep 14;20(1):425. doi: 10.1186/s12891-019-2813-8.
Gout in spine is rare and commonly mimics some infectious or tumoral lesions, the differentiation of spinal gout from other diseases is not always easy. We report a case of gout involved cervical disc and adjacent vertebral endplates whose etiology was initially not determined. Compared with the previous published 10 similar cases, this case displayed a complete and continuous image data with higher image quality and resolution than before. So we give a brief literature review for concerning cervical gout, with the emphasis on the discussion of radiological findings.
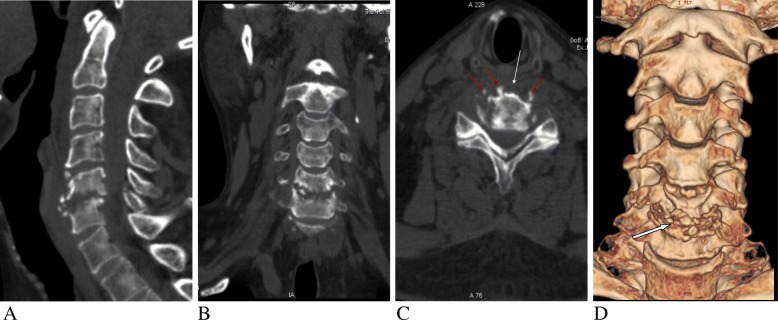
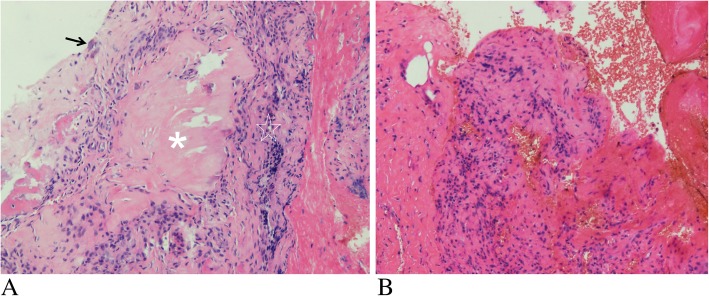
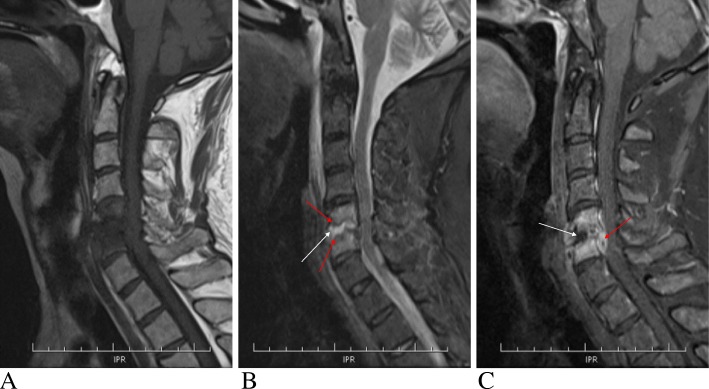
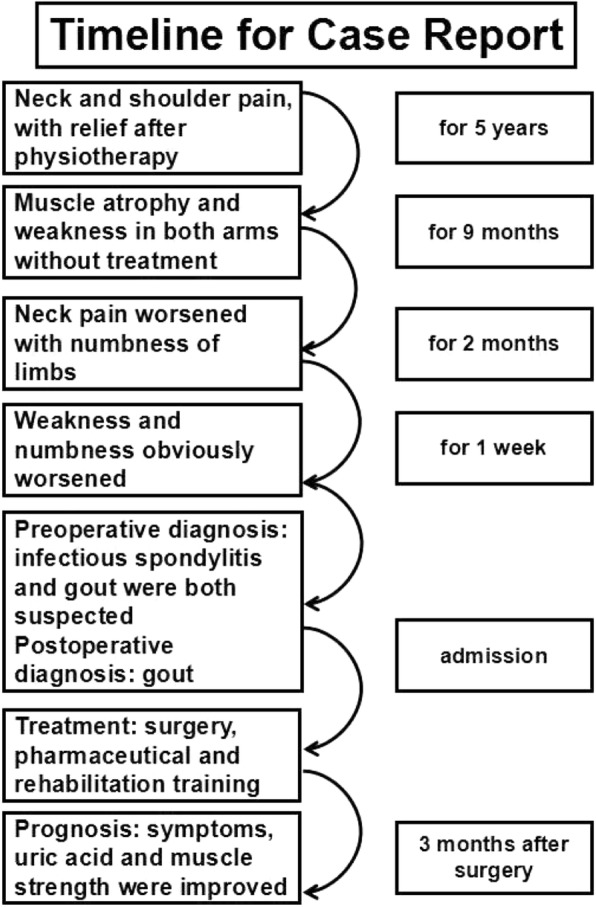
A 50-year-old male with a 5-year history of neck and shoulder pain had muscle atrophy and weakness in both arms. Physical examination revealed multiple tophi were seen in left wrist, both feet and knee; bilateral superficial sensory declined below level of mastoid portion and the muscle strengths of limbs decreased. Laboratory findings showed hyperuricemia and the C-reactive protein level was very high. Imaging studies including Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) showed abnormality of the C5-6 intervertebral disc and irregular osteolytic destruction of both adjacent C5-6 endplates, narrowing of C5-6 disc space and swelling of prevertebral soft tissue. Under the circumstance of the lesions being not determined and nerve root symptoms, surgical treatment was performed and pathological examination of the specimen revealed deposited uric acid crystals surrounded by granulomatous inflammation. After surgery combined with pharmaceutical and rehabilitation treatment, the muscle strengths of limbs, the pain of neck and shoulder and the level of serum uric acid were all improved.
Cervical spinal gout involving the disc and adjacent vertebral endplates is uncommon and may misunderstand infectious spondylodiscitis. Physician and radiologist should take the gouty spondylitis into account with a combination with previous history and clinical manifestations when encountering with such this condition.
脊柱痛风很少见,常模仿一些感染或肿瘤病变,脊柱痛风与其他疾病的鉴别并不总是容易的。我们报告了一例累及颈椎间盘和相邻椎体终板的痛风病例,其病因最初未确定。与之前发表的 10 例类似病例相比,该病例显示了完整和连续的图像数据,图像质量和分辨率更高。因此,我们对相关颈椎痛风进行了简要的文献复习,重点讨论了影像学表现。
一名 50 岁男性,有 5 年颈肩部疼痛史,有双上肢肌肉萎缩和无力。体格检查发现左手腕、双脚和膝盖多处痛风石;双侧浅感觉减退至乳突以下水平,四肢肌力下降。实验室检查显示血尿酸升高,C 反应蛋白水平非常高。影像学检查包括计算机断层扫描(CT)和磁共振成像(MRI)显示 C5-6 椎间盘异常,相邻 C5-6 椎体终板不规则溶骨性破坏,C5-6 椎间盘间隙变窄,椎前软组织肿胀。在病变未确定和神经根症状的情况下,进行了手术治疗,标本的病理检查显示尿酸盐晶体沉积,周围有肉芽肿性炎症。术后结合药物和康复治疗,四肢肌力、颈肩部疼痛和血尿酸水平均得到改善。
累及椎间盘和相邻椎体终板的颈椎痛风少见,可能误诊为感染性脊椎炎。当遇到这种情况时,医生和放射科医生应结合既往病史和临床表现,考虑痛风性脊椎炎。