Huntsman Cancer Institute, University of Utah, Salt Lake City, Utah.
Department of Internal Medicine, University of Utah, Salt Lake City, Utah.
Cancer Med. 2019 Nov;8(15):6789-6798. doi: 10.1002/cam4.2534. Epub 2019 Sep 18.
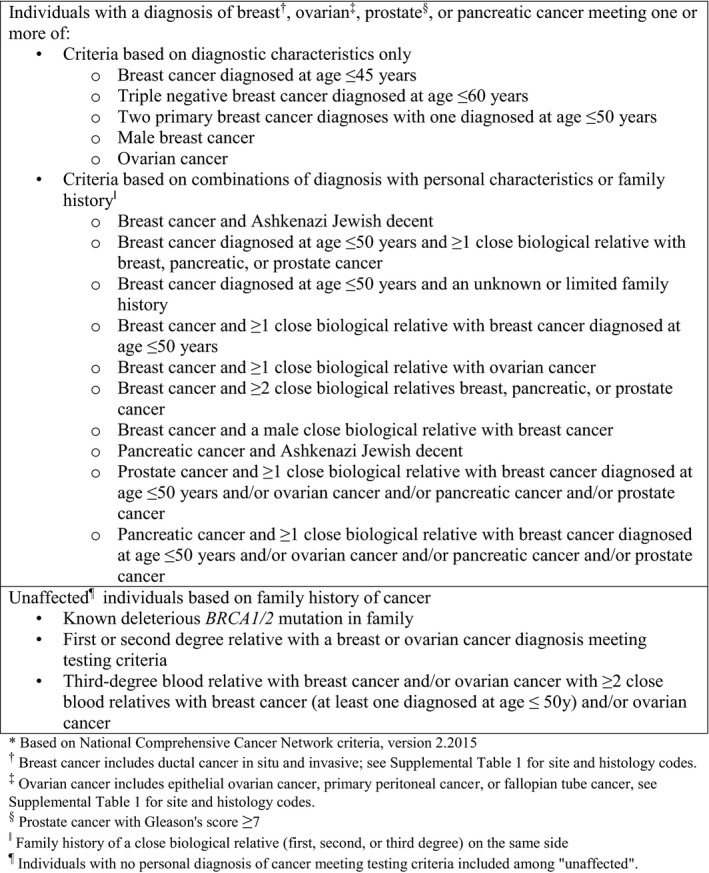
Personal cancer diagnosis and family cancer history factor into which individuals should undergo genetic testing for hereditary breast and ovarian cancer (HBOC) syndrome. Family history is often determined in the research setting through kindreds with disease clusters, or clinically from self-report. The population prevalence of individuals with diagnostic characteristics and/or family cancer history meeting criteria for HBOC testing is unknown.
Utilizing Surveillance, Epidemiology, and End Results (SEER) cancer registry data and a research resource linking registry records to genealogies, the Utah Population Database, the population-based prevalence of diagnostic and family history characteristics meeting National Comprehensive Cancer Network (NCCN) criteria for HBOC testing was objectively assessed.
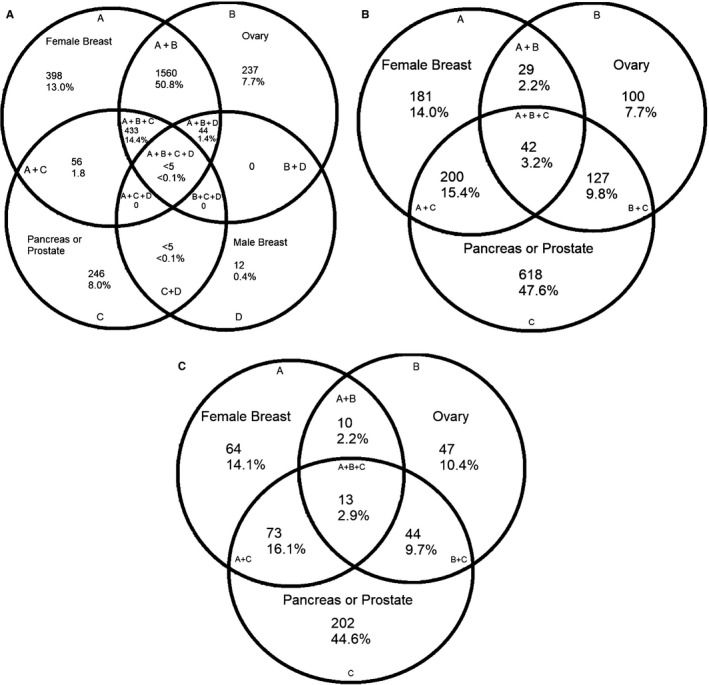
Among Utah residents with an incident breast cancer diagnosis 2010-2015 and evaluable for family history, 21.6% met criteria for testing based on diagnostic characteristics, but the proportion increased to 62.9% when family history was evaluated. The proportion of cases meeting testing criteria at diagnosis was 94% for ovarian cancer, 23% for prostate cancer, and 51.1% for pancreatic cancer. Among an unaffected Utah population of approximately 1.7 million evaluable for family history, 197,601 or 11.6% met testing criteria based on family history.
This study quantifies the population-based prevalence of HBOC criteria using objectively determined genealogy and cancer incidence data. Sporadic breast cancer likely represents a portion of the high prevalence of family cancer history seen in this study. These results underline the importance of establishing presence of a deleterious mutation in an affected family member, per NCCN guidelines, before testing unaffected relatives.
个人癌症诊断和家族癌症史是个体是否应接受遗传性乳腺癌和卵巢癌(HBOC)综合征基因检测的因素。家族史通常通过具有疾病聚集的家族在研究环境中确定,或者通过自我报告在临床环境中确定。具有诊断特征和/或家族癌症史的个体符合 HBOC 检测标准的人群流行率尚不清楚。
利用监测、流行病学和最终结果(SEER)癌症登记数据以及将登记记录与家谱联系起来的研究资源——犹他州人口数据库,客观评估了符合国家综合癌症网络(NCCN)HBOC 检测标准的诊断和家族史特征的人群流行率。
在 2010 年至 2015 年患有乳腺癌且可评估家族史的犹他州居民中,21.6%符合基于诊断特征的检测标准,但在评估家族史时,这一比例增加到 62.9%。在诊断时符合检测标准的病例比例为卵巢癌 94%、前列腺癌 23%和胰腺癌 51.1%。在大约 170 万可评估家族史的未受影响的犹他州人群中,197601 人或 11.6%符合基于家族史的检测标准。
本研究使用客观确定的家谱和癌症发病率数据量化了基于人群的 HBOC 标准流行率。散发性乳腺癌可能代表了本研究中所见家族癌症史高发率的一部分。这些结果强调了按照 NCCN 指南,在检测未受影响的亲属之前,在受影响的家族成员中确定存在有害突变的重要性。