Department of Anesthesiology, Jiangxi Maternal and Child Health Hospital, Nanchang, China.
Department of Anesthesiology, HwaMei Hospital, University of Chinese Academy of Sciences, No.41 Xibei Road, Haishu District, Ningbo, Zhejiang Province, China.
BMC Cancer. 2019 Sep 18;19(1):931. doi: 10.1186/s12885-019-6143-x.
A high prevalence of postoperative complications is closely associated with a worse short- and long-term outcome. This current study aimed to investigate potential risk factors including albumin-to-fibrinogen ratio (AFR) for severe postoperative complications (SPCs) in surgical gastric cancer (GC) patients.
Elderly patients (≥65 years) with primary GC who underwent elective radical laparoscopic gastrectomy under general anesthesia were included. According to the Clavien-Dindo classification system, the severity of complications was assessed from Grade I to V and SPCs were defined as C-D Grade ≥ IIIa. The clinicopathological features, operative-associated characteristics, postoperative recovery and laboratory tests were compared between patients with or without SPCs. Receiver operating characteristic (ROC) curve analysis using Youden's Index was established for determining the predictive value and cut-off threshold of AFR for SPCs. Binary univariate and multivariate logistic regression models were used to assess factors influencing SPCs.
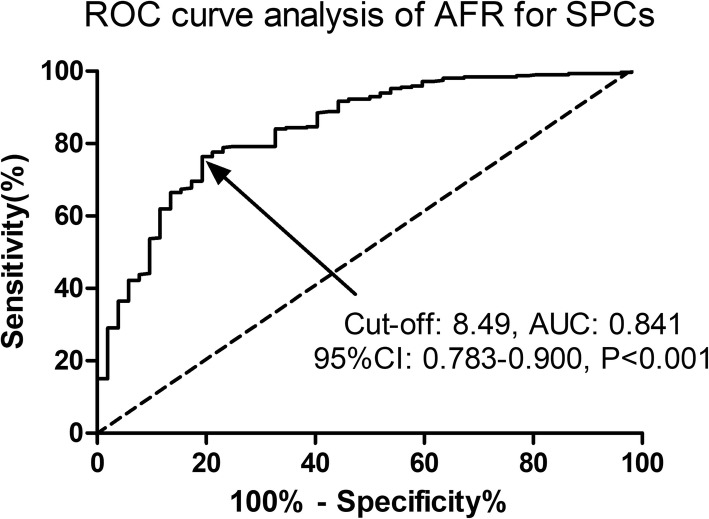
A total of 365 elderly GC patients were finally included in the analysis, of which 52 (52/365, 14.2%) patients had developed SPCs within postoperative 30 days. Preoperative AFR level predicted SPCs in surgical GC patients with an AUC of 0.841, a sensitivity of 76.36% and a specificity of 80.77%, respectively (P < 0.001). The multivariate analysis revealed that a lower AFR level (OR: 1.94, 95% CI: 1.09-3.36, P = 0.017) and an older age (OR: 1.81, 95% CI: 1.06-3.04, P = 0.023) were two independent predictive factors for SPCs in surgical GC patients.
Preoperative AFR level is a useful predictor for SPCs in elderly GC subjects after radical laparoscopic gastrectomy.
术后并发症高发与短期和长期预后不良密切相关。本研究旨在探讨白蛋白-纤维蛋白原比值(AFR)等潜在危险因素,以预测接受全麻下腹腔镜根治性胃切除术的老年胃癌(GC)患者术后发生严重并发症(SPC)的风险。
纳入年龄≥65 岁、接受全麻下腹腔镜根治性胃切除术的原发性 GC 老年患者。根据 Clavien-Dindo 分级系统,对并发症严重程度进行评估,分为 I 至 V 级,SPC 定义为 C-D 分级≥Ⅲa 级。比较 SPC 组与非 SPC 组患者的临床病理特征、手术相关特征、术后恢复情况和实验室检查结果。采用约登指数建立受试者工作特征(ROC)曲线分析,以确定 AFR 预测 SPC 的价值和截断值。采用二项式单因素和多因素逻辑回归模型评估影响 SPC 的因素。
共纳入 365 例老年 GC 患者,其中 52 例(52/365,14.2%)患者术后 30 天内发生 SPC。术前 AFR 水平对老年 GC 患者术后 SPC 有预测价值,AUC 为 0.841,灵敏度为 76.36%,特异度为 80.77%(P<0.001)。多因素分析显示,较低的 AFR 水平(OR:1.94,95%CI:1.09-3.36,P=0.017)和年龄较大(OR:1.81,95%CI:1.06-3.04,P=0.023)是老年 GC 患者术后发生 SPC 的两个独立预测因素。
术前 AFR 水平是预测老年 GC 患者接受腹腔镜根治性胃切除术后 SPC 的有用指标。