Nieuwenburg Stella A V, Waddingham William W, Graham David, Rodriguez-Justo Manuel, Biermann Katharina, Kuipers Ernst J, Banks Matthew, Jansen Marnix, Spaander Manon C W
Gastroenterology & Hepatology, Erasmus MC University Medical Center, Rotterdam, The Netherlands.
Endoscopy, University College London Hospital, London, UK.
BMJ Open. 2019 Sep 18;9(9):e032013. doi: 10.1136/bmjopen-2019-032013.
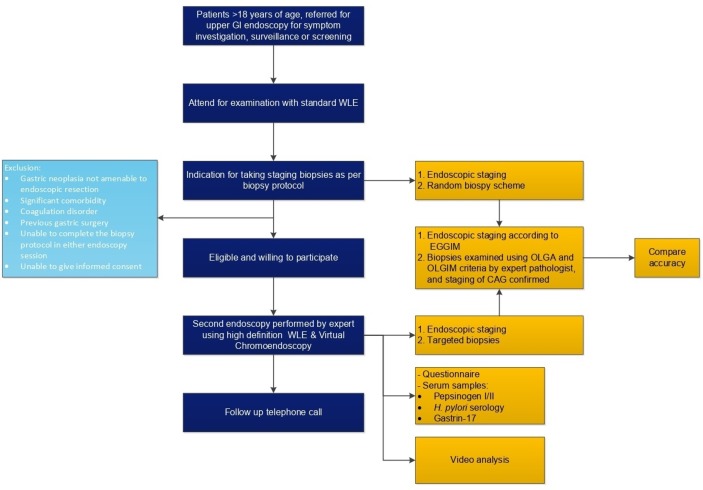
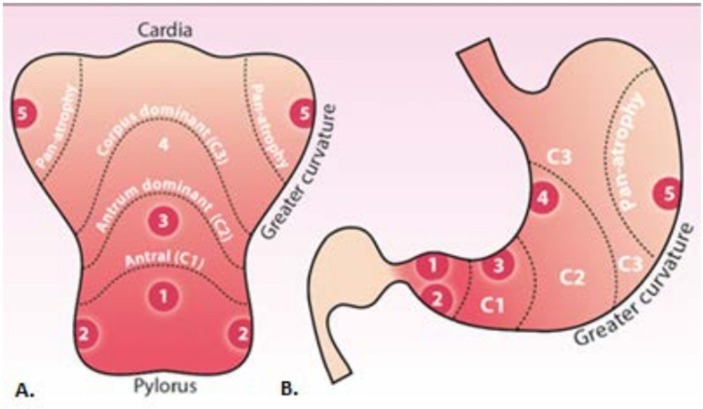
Patients with chronic atrophic gastritis (CAG) and intestinal metaplasia (IM) are at risk of developing gastric adenocarcinoma. Their diagnosis and management currently rely on histopathological guidance after random endoscopic biopsy sampling (Sydney biopsy strategy). This approach has significant flaws such as under-diagnosis, poor reproducibility and poor correlation between endoscopy and histology. This prospective, international multicentre study aims to establish whether endoscopy-led risk stratification accurately and reproducibly predicts CAG and IM extent and disease stage.
Patients with CAG and/or IM on standard white light endoscopy (WLE) will be prospectively identified and invited to undergo a second endoscopy performed by an expert endoscopist using enhanced endoscopic imaging techniques with virtual chromoendoscopy. Extent of CAG/IM will be endoscopically staged with enhanced imaging and compared with standard WLE. Histopathological risk stratification through targeted biopsies will be compared with endoscopic disease staging and to random biopsy staging on WLE as a reference. At least 234 patients are required to show a 10 % difference in sensitivity and accuracy between enhanced imaging endoscopy-led staging and the current biopsy-led staging protocol of gastric atrophy with a power (beta) of 80 % and a 0.05 probability of a type I error (alpha).
The study was approved by the respective Institutional Review Boards (Netherlands: MEC-2018-078; UK: 19/LO/0089). The findings will be published in peer-reviewed journals and presented at scientific meetings.
NTR7661; Pre-results.
慢性萎缩性胃炎(CAG)和肠化生(IM)患者有发生胃腺癌的风险。目前,他们的诊断和管理依赖于随机内镜活检采样后的组织病理学指导(悉尼活检策略)。这种方法存在显著缺陷,如诊断不足、可重复性差以及内镜检查与组织学之间的相关性不佳。这项前瞻性国际多中心研究旨在确定内镜引导下的风险分层能否准确且可重复地预测CAG和IM的范围及疾病分期。
将前瞻性地识别出在标准白光内镜检查(WLE)中有CAG和/或IM的患者,并邀请他们接受由专家内镜医师使用虚拟染色内镜等增强内镜成像技术进行的第二次内镜检查。将通过增强成像对CAG/IM的范围进行内镜分期,并与标准WLE进行比较。通过靶向活检进行的组织病理学风险分层将与内镜疾病分期以及以WLE上的随机活检分期作为参考进行比较。至少需要234名患者,以显示增强成像内镜引导分期与当前胃萎缩活检引导分期方案在敏感性和准确性上有10%的差异,检验效能(β)为80%,I型错误概率(α)为0.05。
该研究已获得各自机构审查委员会的批准(荷兰:MEC - 2018 - 078;英国:19/LO/0089)。研究结果将发表在同行评审期刊上,并在科学会议上展示。
NTR7661;预结果。