Department of Emergency Medicine, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, 310016, China.
Department of Surgery, Wound Care Clinical Research Program, boston University School of Medicine and Boston Medical Center, Boston, MA, 02118, USA.
Sci Rep. 2019 Sep 20;9(1):13644. doi: 10.1038/s41598-019-50178-0.
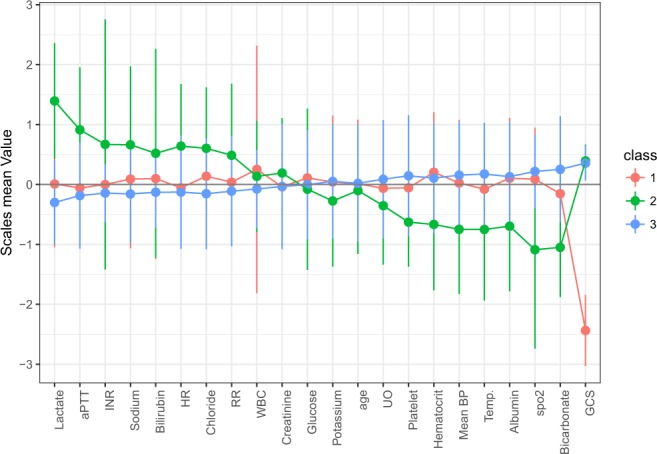
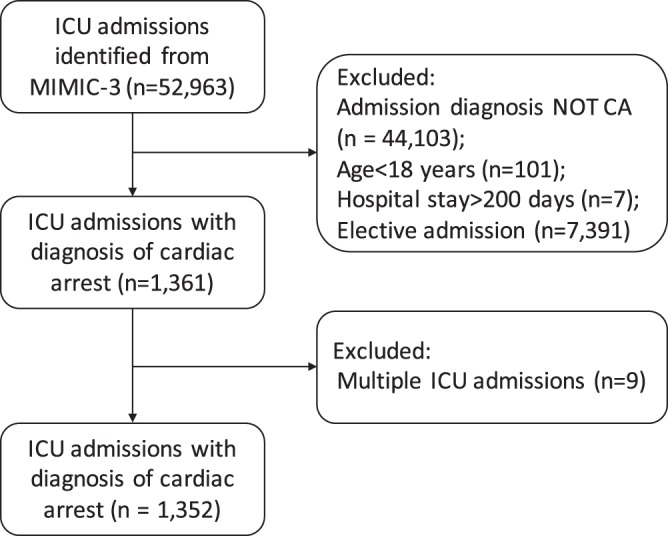
Cardiac arrest (CA) may occur due to a variety of causes with heterogeneity in their clinical presentation and outcomes. This study aimed to identify clinical patterns or subphenotypes of CA patients admitted to the intensive care unit (ICU). The clinical and laboratory data of CA patients in a large electronic healthcare database were analyzed by latent profile analysis (LPA) to identify whether subphenotypes existed. Multivariable Logistic regression was used to assess whether mortality outcome was different between subphenotypes. A total of 1,352 CA patients fulfilled the eligibility criteria were included. The LPA identified three distinct subphenotypes: Profile 1 (13%) was characterized by evidence of significant neurological injury (low GCS). Profile 2 (15%) was characterized by multiple organ dysfunction with evidence of coagulopathy (prolonged aPTT and INR, decreased platelet count), hepatic injury (high bilirubin), circulatory shock (low mean blood pressure and elevated serum lactate); Profile 3 was the largest proportion (72%) of all CA patients without substantial derangement in major organ function. Profile 2 was associated with a significantly higher risk of death (OR: 2.09; 95% CI: 1.30 to 3.38) whilst the mortality rates of Profiles 3 was not significantly different from Profile 1 in multivariable model. LPA using routinely collected clinical data could identify three distinct subphenotypes of CA; those with multiple organ failure were associated with a significantly higher risk of mortality than other subphenotypes. LPA profiling may help researchers to identify the most appropriate subphenotypes of CA patients for testing effectiveness of a new intervention in a clinical trial.
心脏骤停 (CA) 可能由多种原因引起,其临床表现和结局存在异质性。本研究旨在确定入住重症监护病房 (ICU) 的 CA 患者的临床模式或亚表型。通过潜在剖面分析 (LPA) 对大型电子医疗保健数据库中 CA 患者的临床和实验室数据进行分析,以确定是否存在亚表型。多变量逻辑回归用于评估亚表型之间的死亡率是否不同。共纳入 1352 名符合入选标准的 CA 患者。LPA 确定了三个不同的亚表型:表型 1(13%)的特征是有明显的神经损伤证据(低 GCS)。表型 2(15%)的特征是多器官功能障碍,伴有凝血功能障碍(延长 aPTT 和 INR、血小板计数降低)、肝损伤(高胆红素)、循环休克(平均血压低和血清乳酸升高)的证据;表型 3 是所有 CA 患者中比例最大(72%)的,主要器官功能没有明显紊乱。表型 2与死亡风险显著增加相关(OR:2.09;95%CI:1.30 至 3.38),而多变量模型中表型 3 的死亡率与表型 1 无显著差异。使用常规收集的临床数据进行 LPA 可以识别 CA 的三个不同亚表型;那些伴有多器官衰竭的患者与其他亚表型相比,死亡风险显著增加。LPA 分析可能有助于研究人员为临床试验中测试新干预措施的有效性,确定 CA 患者最合适的亚表型。