Dept. of Pharmacology, Institute of Post Graduate Medical Education and Research, Kolkata, 700020, India.
Dept. of Microbiology, Govt. Medical College, Purulia, India.
Int J Parasitol Drugs Drug Resist. 2019 Dec;11:166-176. doi: 10.1016/j.ijpddr.2019.08.005. Epub 2019 Aug 22.
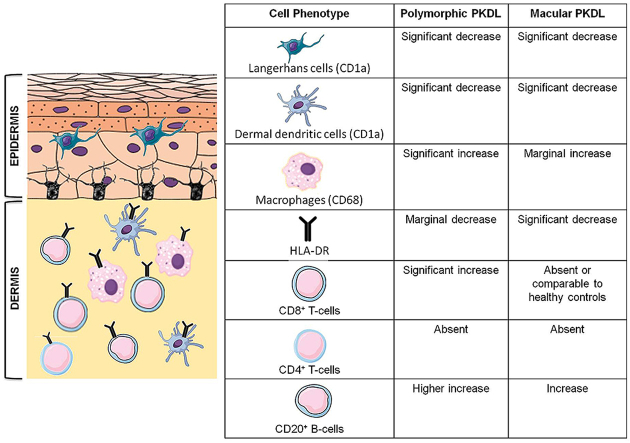
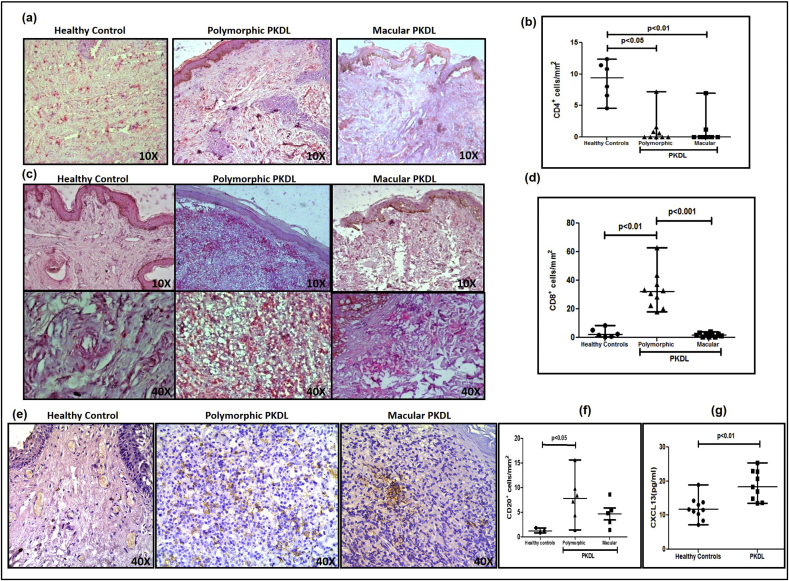
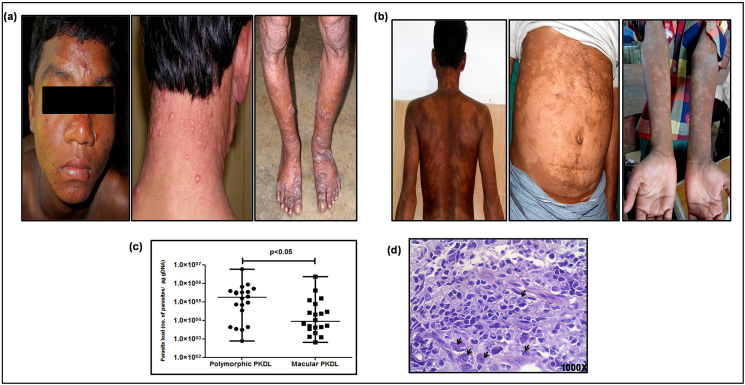
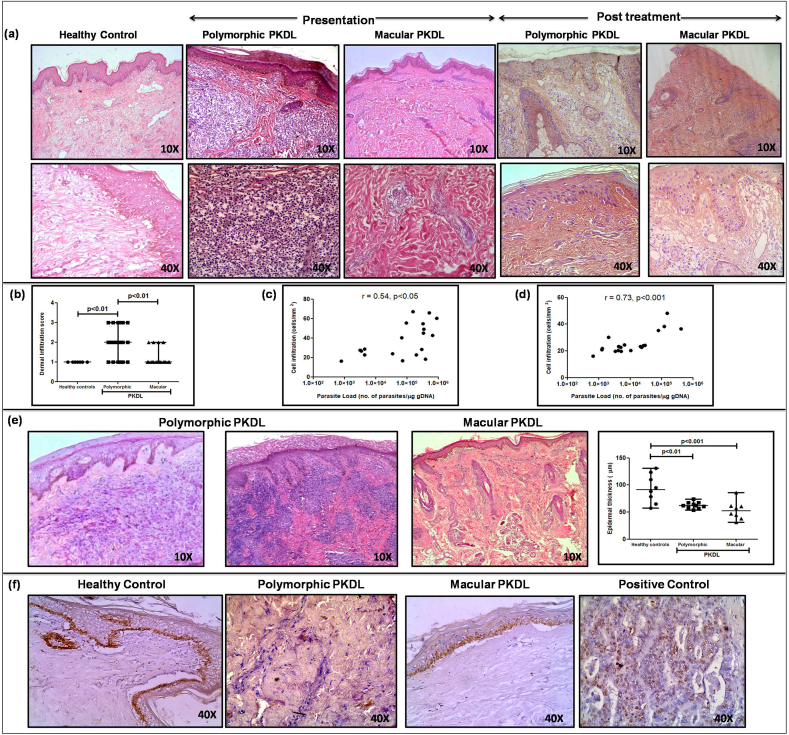
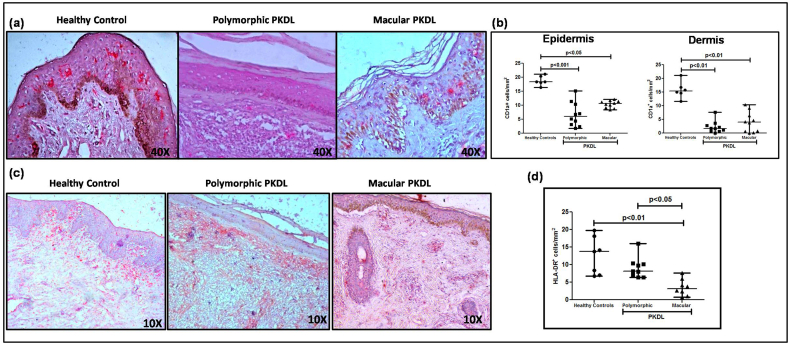
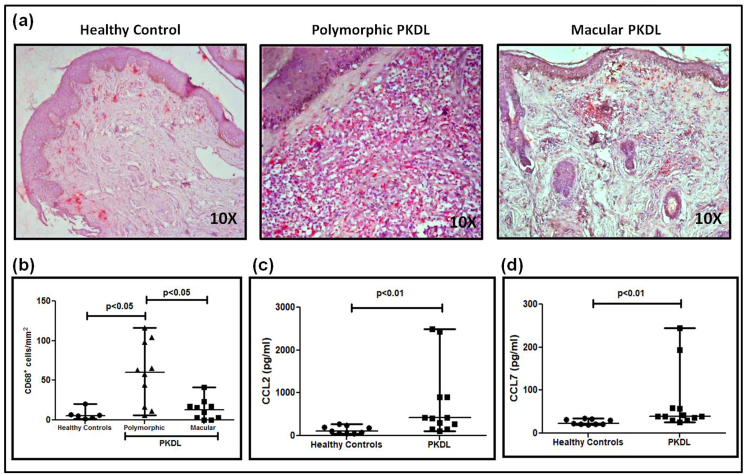
Post Kala-azar Dermal Leishmaniasis (PKDL), a sequel of apparently cured Visceral Leishmaniasis presents in South Asia with papulonodular (polymorphic) or hypomelanotic lesions (macular). Till date, the polymorphic variant was considered predominant, constituting 85-90%. However, following active-case surveillance, the proportion of macular PKDL has increased substantially to nearly 50%, necessitating an in-depth analysis of this variant. Accordingly, this study aimed to delineate the cellular infiltrate in macular vis-à-vis polymorphic PKDL. To study the overall histopathology, hematoxylin and eosin staining was performed on lesional sections and phenotyping by immunohistochemistry done in terms of dendritic cells (CD1a), macrophages (CD68), HLA-DR, T-cells (CD8, CD4), B-cells (CD20) and Ki67 along with assessment of the status of circulating homing markers CCL2, CCL7 and CXCL13. In polymorphic cases (n = 20), the cellular infiltration was substantial, whereas in macular lesions (n = 20) it was mild and patchy with relative sparing of the reticular dermis. Although parasite DNA was identified in both variants by ITS-1 PCR, the parasite load was significantly higher in the polymorphic variant and Leishman-Donovan bodies were notably minimally present in macular cases. Both variants demonstrated a decrease in CD1a dendritic cells, HLA-DR expression and CD4 T-cells. In macular cases, the proportion of CD68 macrophages, CD8 T-cells and CD20 B-cells was 4.6 fold, 17.0 fold and 1.6 fold lower than polymorphic cases. The absence of Ki67 positivity and increased levels of chemoattractants suggested dermal homing of these cellular subsets. Taken together, as compared to the polymorphic variant, patients with macular PKDL demonstrated a lower parasite load along with a lesser degree of cellular infiltration, suggesting differences in host-pathogen interactions, which in turn can impact on their disease transmitting potential and responses to chemotherapy.
皮肤利什曼病(PKDL)是内脏利什曼病治愈后的一种后遗症,在南亚表现为丘疹结节(多形性)或色素减退性(斑片状)病变。直到目前为止,多形性变异体被认为是主要形式,占 85-90%。然而,随着主动病例监测的进行,斑片状 PKDL 的比例大幅增加,几乎达到 50%,这需要对这种变异体进行深入分析。因此,本研究旨在描绘斑片状和多形性 PKDL 中的细胞浸润。为了研究整体组织病理学,对病变部位进行了苏木精和伊红染色,并通过免疫组织化学进行了表型分析,包括树突细胞(CD1a)、巨噬细胞(CD68)、HLA-DR、T 细胞(CD8、CD4)、B 细胞(CD20)和 Ki67,并评估循环归巢标志物 CCL2、CCL7 和 CXCL13 的状态。在多形性病例(n=20)中,细胞浸润明显,而在斑片状病变中(n=20),细胞浸润较轻且呈斑片状,网状真皮相对保留。尽管在两种变异体中均通过 ITS-1 PCR 鉴定出寄生虫 DNA,但多形性变异体中的寄生虫负荷明显更高,而斑片状病例中明显很少存在利什曼- Donovan 体。两种变异体均表现出 CD1a 树突状细胞、HLA-DR 表达和 CD4 T 细胞减少。在斑片状病例中,CD68 巨噬细胞、CD8 T 细胞和 CD20 B 细胞的比例分别比多形性病例低 4.6 倍、17.0 倍和 1.6 倍。Ki67 阳性率降低和趋化因子水平升高提示这些细胞亚群向真皮归巢。总的来说,与多形性变异体相比,斑片状 PKDL 患者的寄生虫负荷较低,细胞浸润程度较低,提示宿主-病原体相互作用存在差异,这反过来又会影响其疾病传播潜力和对化疗的反应。