Lewis Gemma, Duffy Larisa, Ades Anthony, Amos Rebekah, Araya Ricardo, Brabyn Sally, Button Katherine S, Churchill Rachel, Derrick Catherine, Dowrick Christopher, Gilbody Simon, Fawsitt Christopher, Hollingworth William, Jones Vivien, Kendrick Tony, Kessler David, Kounali Daphne, Khan Naila, Lanham Paul, Pervin Jodi, Peters Tim J, Riozzie Derek, Salaminios George, Thomas Laura, Welton Nicky J, Wiles Nicola, Woodhouse Rebecca, Lewis Glyn
Division of Psychiatry, University College London, London, UK.
Division of Psychiatry, University College London, London, UK.
Lancet Psychiatry. 2019 Nov;6(11):903-914. doi: 10.1016/S2215-0366(19)30366-9. Epub 2019 Sep 19.
Depression is usually managed in primary care, but most antidepressant trials are of patients from secondary care mental health services, with eligibility criteria based on diagnosis and severity of depressive symptoms. Antidepressants are now used in a much wider group of people than in previous regulatory trials. We investigated the clinical effectiveness of sertraline in patients in primary care with depressive symptoms ranging from mild to severe and tested the role of severity and duration in treatment response.
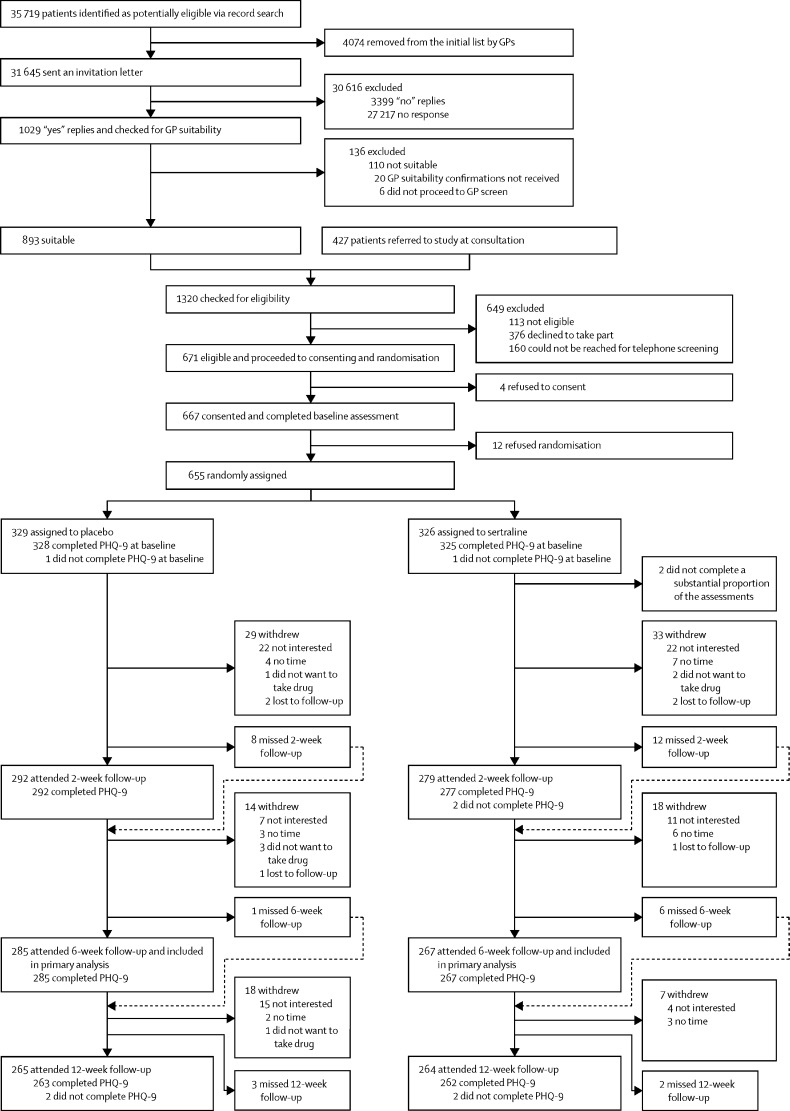
The PANDA study was a pragmatic, multicentre, double-blind, placebo-controlled randomised trial of patients from 179 primary care surgeries in four UK cities (Bristol, Liverpool, London, and York). We included patients aged 18 to 74 years who had depressive symptoms of any severity or duration in the past 2 years, where there was clinical uncertainty about the benefit of an antidepressant. This strategy was designed to improve the generalisability of our sample to current use of antidepressants within primary care. Patients were randomly assigned (1:1) with a remote computer-generated code to sertraline or placebo, and were stratified by severity, duration, and site with random block length. Patients received one capsule (sertraline 50 mg or placebo orally) daily for one week then two capsules daily for up to 11 weeks, consistent with evidence on optimal dosages for efficacy and acceptability. The primary outcome was depressive symptoms 6 weeks after randomisation, measured by Patient Health Questionnaire, 9-item version (PHQ-9) scores. Secondary outcomes at 2, 6 and 12 weeks were depressive symptoms and remission (PHQ-9 and Beck Depression Inventory-II), generalised anxiety symptoms (Generalised Anxiety Disorder Assessment 7-item version), mental and physical health-related quality of life (12-item Short-Form Health Survey), and self-reported improvement. All analyses compared groups as randomised (intention-to-treat). The study is registered with EudraCT, 2013-003440-22 (protocol number 13/0413; version 6.1) and ISRCTN, ISRCTN84544741, and is closed to new participants.
Between Jan 1, 2015, and Aug 31, 2017, we recruited and randomly assigned 655 patients-326 (50%) to sertraline and 329 (50%) to placebo. Two patients in the sertraline group did not complete a substantial proportion of the baseline assessment and were excluded, leaving 653 patients in total. Due to attrition, primary outcome analyses were of 550 patients (266 in the sertraline group and 284 in the placebo group; 85% follow-up that did not differ by treatment allocation). We found no evidence that sertraline led to a clinically meaningful reduction in depressive symptoms at 6 weeks. The mean 6-week PHQ-9 score was 7·98 (SD 5·63) in the sertraline group and 8·76 (5·86) in the placebo group (adjusted proportional difference 0·95, 95% CI 0·85-1·07; p=0·41). However, for secondary outcomes, we found evidence that sertraline led to reduced anxiety symptoms, better mental (but not physical) health-related quality of life, and self-reported improvements in mental health. We observed weak evidence that depressive symptoms were reduced by sertraline at 12 weeks. We recorded seven adverse events-four for sertraline and three for placebo, and adverse events did not differ by treatment allocation. Three adverse events were classified as serious-two in the sertraline group and one in the placebo group. One serious adverse event in the sertraline group was classified as possibly related to study medication.
Sertraline is unlikely to reduce depressive symptoms within 6 weeks in primary care but we observed improvements in anxiety, quality of life, and self-rated mental health, which are likely to be clinically important. Our findings support the prescription of SSRI antidepressants in a wider group of participants than previously thought, including those with mild to moderate symptoms who do not meet diagnostic criteria for depression or generalised anxiety disorder.
National Institute for Health Research.
抑郁症通常在初级保健机构中进行管理,但大多数抗抑郁药物试验的对象是来自二级保健心理健康服务机构的患者,其纳入标准基于抑郁症状的诊断和严重程度。与以往的监管试验相比,现在使用抗抑郁药物的人群要广泛得多。我们调查了舍曲林在初级保健机构中症状轻重不一的抑郁症患者中的临床疗效,并测试了症状严重程度和病程在治疗反应中的作用。
PANDA研究是一项实用的、多中心的、双盲的、安慰剂对照的随机试验,研究对象来自英国四个城市(布里斯托尔、利物浦、伦敦和约克)的179家初级保健诊所。我们纳入了年龄在18至74岁之间、在过去两年中出现过任何严重程度或病程的抑郁症状且临床对使用抗抑郁药物的益处存在不确定性的患者。这一策略旨在提高我们的样本对初级保健机构中当前抗抑郁药物使用情况的代表性。患者通过远程计算机生成的代码以1:1的比例随机分配至舍曲林组或安慰剂组,并按严重程度、病程和地点分层,随机分组长度不等。患者每天服用一粒胶囊(舍曲林50毫克或安慰剂口服),持续一周,然后每天服用两粒胶囊,持续长达11周,这与关于疗效和可接受性的最佳剂量的证据一致。主要结局是随机分组后6周的抑郁症状,通过患者健康问卷9项版(PHQ-9)评分进行测量。2周、6周和12周的次要结局包括抑郁症状和缓解情况(PHQ-9和贝克抑郁量表-II)、广泛性焦虑症状(广泛性焦虑障碍评估7项版)、与身心健康相关的生活质量(12项简短健康调查)以及自我报告的改善情况。所有分析均将分组视为随机分组(意向性分析)。该研究已在欧洲临床试验数据库(EudraCT)注册,注册号为2013-003440-22(方案编号13/0413;版本6.1)以及国际标准随机对照试验编号(ISRCTN),ISRCTN84544741,并且已不再招募新参与者。
在2015年1月1日至2017年8月31日期间,我们招募并随机分配了655名患者——326名(50%)分配至舍曲林组,329名(50%)分配至安慰剂组。舍曲林组有两名患者未完成大部分基线评估,被排除在外,最终共有653名患者。由于失访,主要结局分析纳入了550名患者(舍曲林组266名,安慰剂组284名;85%的随访率,两组间无差异)。我们没有发现证据表明舍曲林在6周时能使抑郁症状出现具有临床意义的减轻。舍曲林组6周时PHQ-9的平均评分为7.98(标准差5.63),安慰剂组为8.76(5.86)(调整后的比例差异为0.95,95%置信区间为0.85 - 1.07;p = 0.41)。然而,对于次要结局,我们发现有证据表明舍曲林能减轻焦虑症状,改善与心理健康(而非身体健康)相关的生活质量,并使自我报告的心理健康状况得到改善。我们观察到有微弱证据表明舍曲林在12周时能减轻抑郁症状。我们记录了7起不良事件——舍曲林组4起,安慰剂组3起,且不良事件在治疗分组间无差异。3起不良事件被归类为严重不良事件——舍曲林组2起,安慰剂组1起。舍曲林组的1起严重不良事件被归类为可能与研究药物有关。
在初级保健机构中,舍曲林不太可能在6周内减轻抑郁症状,但我们观察到其在焦虑、生活质量和自我评定的心理健康方面有所改善,这些可能具有重要的临床意义。我们的研究结果支持在比以往认为的更广泛的参与者群体中开具选择性5-羟色胺再摄取抑制剂(SSRI)类抗抑郁药物,包括那些有轻度至中度症状但不符合抑郁症或广泛性焦虑障碍诊断标准的患者。
英国国家卫生研究院。