Department of Population Health, London School of Hygiene and Tropical Medicine, London, UK.
Ipas, Chapel Hill, NC, USA.
Glob Health Sci Pract. 2019 Sep 26;7(3):386-403. doi: 10.9745/GHSP-D-19-00015. Print 2019 Sep.
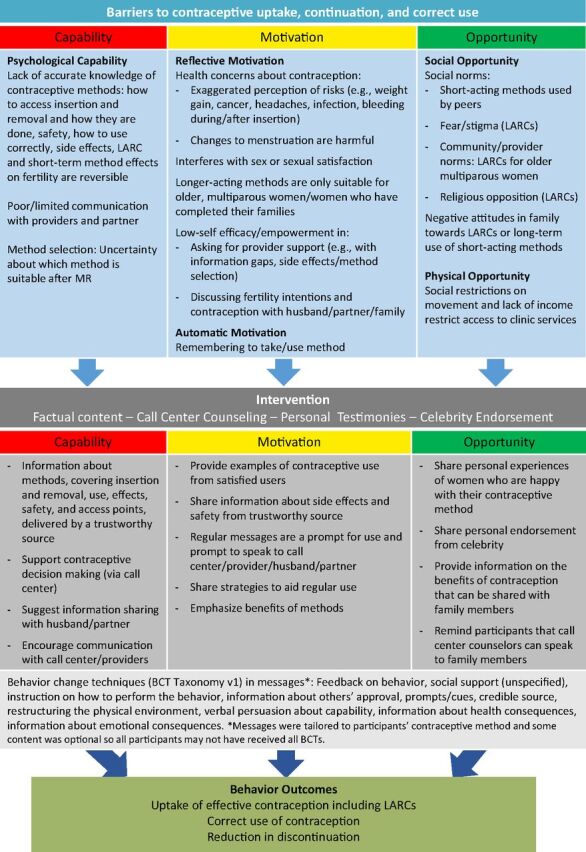
Mobile phones for health (mHealth) hold promise for delivering behavioral interventions. We evaluated the effect of automated interactive voice messages promoting contraceptive use with a focus on long-acting reversible contraceptives (LARCs) among women in Bangladesh who had undergone menstrual regulation (MR), a procedure to "regulate the menstrual cycle when menstruation is absent for a short duration."
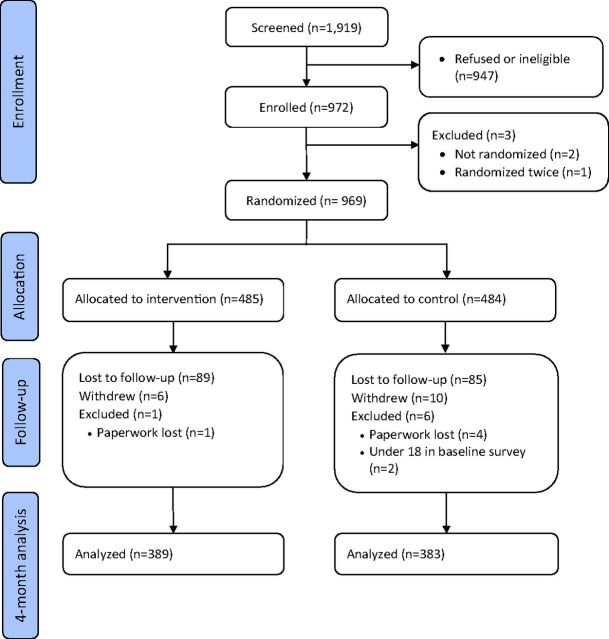
We recruited MR clients from 41 public- and private-sector clinics immediately after MR. Eligibility criteria included having a personal mobile phone and consenting to receive messages about family planning by phone. We randomized participants remotely to an intervention group that received at least 11 voice messages about contraception over 4 months or to a control group (no messages). The primary outcome was LARC use at 4 months. Adverse events measured included experience of intimate partner violence (IPV). Researchers recruiting participants and 1 analyst were blinded to allocation groups. All analyses were intention to treat. The trial is registered with ClinicalTrials.gov (NCT02579785).
Between December 2015 and March 2016, 485 women were allocated to the intervention group and 484 to the control group. We completed follow-up on 389 intervention and 383 control participants. Forty-eight (12%) participants in the intervention group and 59 (15%) in the control group reported using a LARC method at 4 months (adjusted odds ratio [aOR] using multiple imputation=0.95; 95% confidence interval [CI]=0.49 to 1.83; =.22). Reported physical IPV was higher in the intervention group: 42 (11%) intervention versus 25 (7%) control (aOR=1.97; 95% CI=1.12 to 3.46; =.03) when measured using a closed question naming acts of violence. No violence was reported in response to an open question about effects of being in the study.
The intervention did not increase LARC use but had an unintended consequence of increasing self-reported IPV. Researchers and health program designers should consider possible negative impacts when designing and evaluating mHealth and other reproductive health interventions. IPV must be measured using closed questions naming acts of violence.
移动医疗(mHealth)有望提供行为干预措施。我们评估了针对孟加拉国接受过月经调节(MR)的女性的自动交互语音消息在促进避孕措施使用方面的效果,MR 是一种“当月经短暂停止时调节月经周期”的程序。
我们在 MR 后立即从 41 家公立和私立诊所招募 MR 客户。入选标准包括拥有个人移动电话并同意通过电话接收有关计划生育的信息。我们通过远程将参与者随机分配到干预组(至少收到 11 条关于避孕的语音信息,为期 4 个月)或对照组(无消息)。主要结局是 4 个月时使用长效可逆避孕方法(LARC)。测量的不良事件包括亲密伴侣暴力(IPV)的经历。招募参与者的研究人员和 1 位分析人员对分组情况不知情。所有分析均按意向治疗进行。该试验在 ClinicalTrials.gov 注册(NCT02579785)。
2015 年 12 月至 2016 年 3 月,485 名女性被分配到干预组,484 名女性被分配到对照组。我们对 389 名干预组和 383 名对照组参与者进行了随访。在 4 个月时,干预组中有 48(12%)名参与者和对照组中有 59(15%)名参与者报告使用了 LARC 方法(采用多重插补的调整优势比[aOR] = 0.95;95%置信区间[CI] = 0.49 至 1.83;=.22)。当使用封闭问题命名暴力行为时,干预组报告的身体 IPV 更高:42(11%)例干预组与 25(7%)例对照组(调整比值比[aOR]=1.97;95%CI=1.12 至 3.46;=.03)。未在开放问题中报告任何暴力行为,该问题询问参加研究的影响。
该干预措施并未增加 LARC 的使用,但却意外增加了自我报告的 IPV。在设计和评估移动医疗和其他生殖健康干预措施时,研究人员和卫生计划设计者应考虑可能产生的负面影响。必须使用封闭问题命名暴力行为来测量 IPV。