Department of Neurology, George Washington University School of Medicine, Washington, DC, USA.
Global Medical Affairs, Allergan plc, Irvine, CA, USA.
Headache. 2019 Nov;59(10):1700-1713. doi: 10.1111/head.13653. Epub 2019 Sep 26.
To compare effectiveness of onabotulinumtoxinA and topiramate for chronic migraine (CM) prevention.
The efficacy* of onabotulinumtoxinA and topiramate has been established in placebo-controlled randomized clinical trials (defined as the benefit of treatment under ideal conditions). The effectiveness of the 2 preventive treatments, however, has not been established (*the benefit of treatment under real-world conditions, representing a blend of efficacy and tolerability).
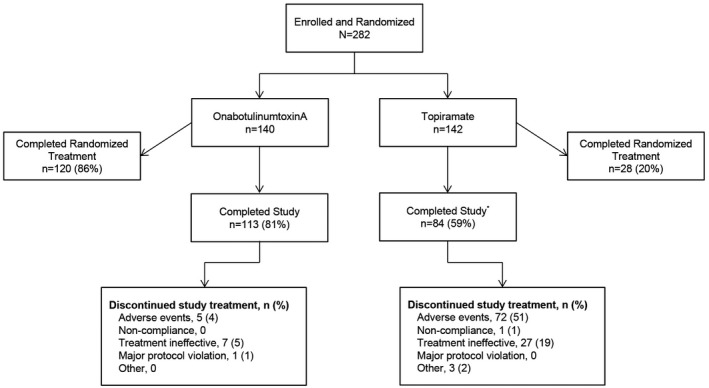
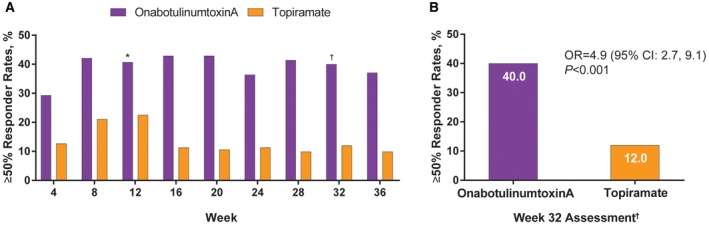
In this multicenter, randomized, parallel-group, post-authorization, open-label prospective study (FORWARD; ClinicalTrials.gov, NCT02191579), we randomized adults with CM (1:1) to onabotulinumtoxinA 155 U every 12 weeks for 3 cycles or topiramate "immediate release" 50-100 mg/day to week 36. Primary outcome measure was proportion of patients achieving ≥50% reduction in headache days (weeks 29-32). Missing values were imputed using baseline observation carried forward (BOCF) methodology. After 12 weeks, patients initially randomized to topiramate could cross over to onabotulinumtoxinA treatment. We monitored and recorded all adverse events (AEs).
We enrolled 282 patients (onabotulinumtoxinA, n = 140; topiramate, n = 142) and 148 patients completed randomized treatment (onabotulinumtoxinA, n = 120 [86%]; topiramate, n = 28 [20%]). Primary reasons for withdrawal were ineffective treatment (onabotulinumtoxinA, n = 7 [5%]; topiramate, n = 27 [19%]) and AEs (onabotulinumtoxinA, n = 5 [4%]; topiramate, n = 72 [51%]). Eighty topiramate patients crossed over to onabotulinumtoxinA. In the BOCF analysis, a significantly higher proportion of patients randomized to onabotulinumtoxinA experienced ≥50% reduction in headache frequency compared with those randomized to topiramate (40% [56/140] vs 12% [17/142], respectively; adjusted OR, 4.9 [95% CI, 2.7-9.1]; P < .001). OnabotulinumtoxinA was superior to topiramate in meeting secondary endpoints. In a post hoc analysis using observed data, the 50% responder rates at week 12 were 45.6% for onabotulinumtoxinA (n = 125) and 29.4% for topiramate (n = 109) (P = .015). AEs were reported by 48% (105/220) of onabotulinumtoxinA and 79% (112/142) of topiramate patients. Results were similar in those who crossed over to onabotulinumtoxinA.
While using imputation methods of accounting for differences in discontinuation rates, we found onabotulinumtoxinA to have greater clinical utility than topiramate, largely because of tolerability issues associated with the latter and a relatively higher number of onabotulinumtoxinA patients remaining on treatment.
比较肉毒毒素 A 与托吡酯预防慢性偏头痛(CM)的效果。
肉毒毒素 A 和托吡酯的疗效已在安慰剂对照随机临床试验中得到证实(定义为在理想条件下治疗的益处)。然而,这两种预防性治疗的有效性尚未得到证实(在真实世界条件下治疗的益处,代表疗效和耐受性的融合)。
在这项多中心、随机、平行分组、上市后、开放标签前瞻性研究(FORWARD;ClinicalTrials.gov,NCT02191579)中,我们将 CM 成人患者(1:1)随机分为肉毒毒素 A 155 U 每 12 周 1 次,共 3 个周期,或托吡酯“速释”50-100mg/天至第 36 周。主要结局测量指标是头痛天数减少≥50%的患者比例(第 29-32 周)。缺失值采用基线观察结转(BOCF)方法进行估算。12 周后,最初随机分配至托吡酯的患者可交叉至肉毒毒素 A 治疗。我们监测并记录所有不良事件(AE)。
我们共纳入 282 例患者(肉毒毒素 A,n=140;托吡酯,n=142),148 例患者完成了随机治疗(肉毒毒素 A,n=120[86%];托吡酯,n=28[20%])。退出的主要原因是治疗无效(肉毒毒素 A,n=7[5%];托吡酯,n=27[19%])和 AE(肉毒毒素 A,n=5[4%];托吡酯,n=72[51%])。80 例托吡酯患者交叉至肉毒毒素 A。在 BOCF 分析中,与随机分配至托吡酯的患者相比,随机分配至肉毒毒素 A 的患者头痛频率减少≥50%的比例显著更高(分别为 40%[56/140]与 12%[17/142];调整后的 OR,4.9[95%CI,2.7-9.1];P<.001)。肉毒毒素 A 在次要终点方面优于托吡酯。在使用观察数据的事后分析中,肉毒毒素 A 治疗第 12 周的 50%应答率为 45.6%(n=125),托吡酯为 29.4%(n=109)(P=0.015)。48%(220 例中的 105 例)的肉毒毒素 A 患者和 79%(142 例中的 112 例)的托吡酯患者报告了 AE。交叉至肉毒毒素 A 的患者也有类似的结果。
在使用差异辍学率的估算方法时,我们发现肉毒毒素 A 的临床效果优于托吡酯,这主要是由于后者与耐受性问题相关,以及相对较多的肉毒毒素 A 患者继续接受治疗。