Computational and Biological Learning, Department of Engineering, University of Cambridge, Cambridge CB2 1PZ, United Kingdom,
Department of Neuroscience, Physiology and Pharmacology, University College London, London WC1E 6BT, United Kingdom.
J Neurosci. 2019 Nov 13;39(46):9185-9196. doi: 10.1523/JNEUROSCI.2005-18.2019. Epub 2019 Sep 30.
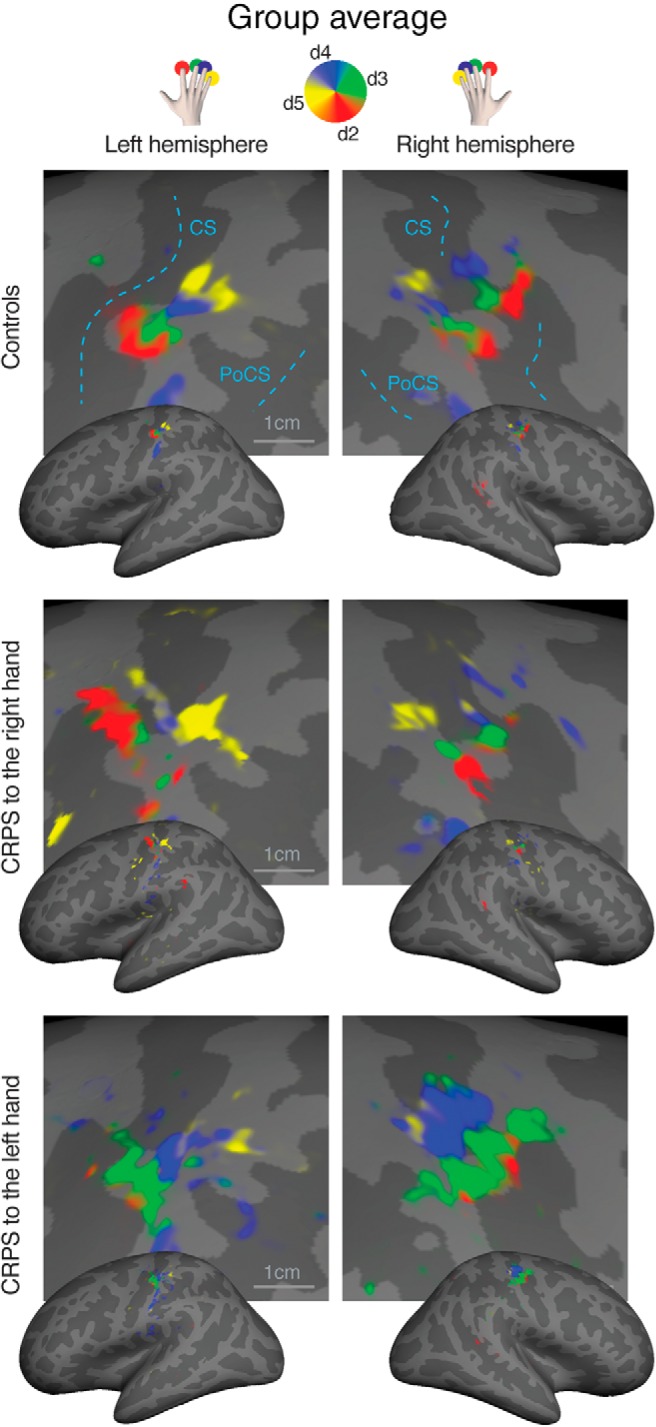
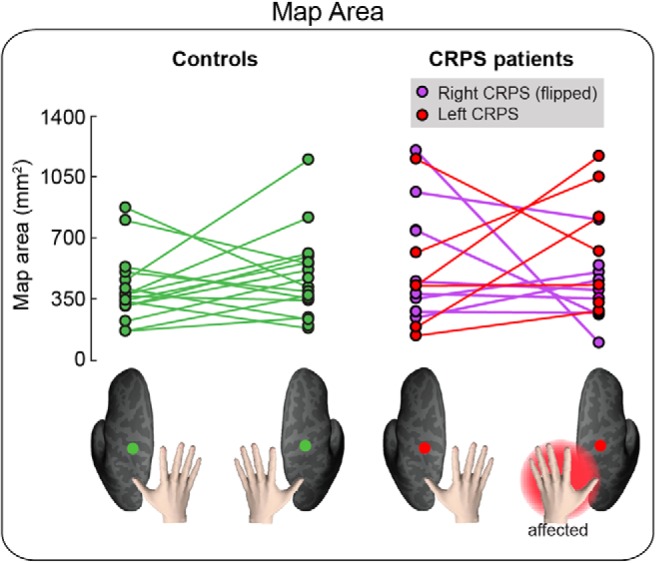
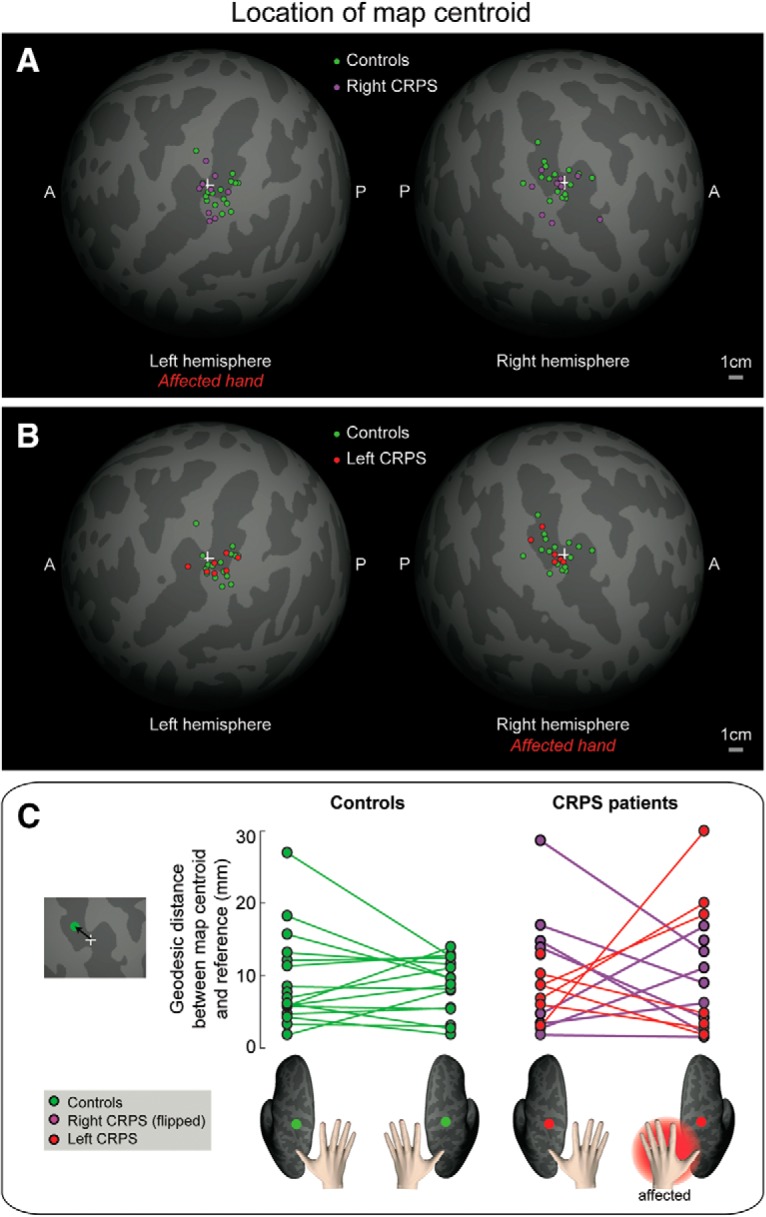
It has long been thought that severe chronic pain conditions, such as complex regional pain syndrome (CRPS), are not only associated with, but even maintained by a reorganization of the somatotopic representation of the affected limb in primary somatosensory cortex (S1). This notion has driven treatments that aim to restore S1 representations in CRPS patients, such as sensory discrimination training and mirror therapy. However, this notion is based on both indirect and incomplete evidence obtained with imaging methods with low spatial resolution. Here, we used fMRI to characterize the S1 representation of the affected and unaffected hand in humans (of either sex) with unilateral CRPS. The cortical area, location, and geometry of the S1 representation of the CRPS hand were largely comparable with those of both the unaffected hand and healthy controls. We found no differential relation between affected versus unaffected hand map measures and clinical measures (pain severity, upper limb disability, disease duration). Thus, if any map reorganization occurs, it does not appear to be directly related to pain and disease severity. These findings compel us to reconsider the cortical mechanisms underlying CRPS and the rationale for interventions that aim to "restore" somatotopic representations to treat pain. This study shows that the spatial map of the fingers in somatosensory cortex is largely preserved in chronic complex regional pain syndrome (CRPS). These findings challenge the treatment rationale for restoring somatotopic representations in complex regional pain syndrome patients.
长期以来,人们一直认为严重的慢性疼痛状况,如复杂性区域疼痛综合征(CRPS),不仅与受影响肢体在初级体感皮层(S1)中的躯体定位代表的重新组织有关,甚至还维持着这种重新组织。这种观念推动了旨在恢复 CRPS 患者 S1 代表的治疗方法,如感觉辨别训练和镜像疗法。然而,这种观念基于使用具有低空间分辨率的成像方法获得的间接和不完整的证据。在这里,我们使用 fMRI 来描述单侧 CRPS 患者的受累和未受累手的 S1 代表。CRPS 手的 S1 代表的皮质区域、位置和几何形状在很大程度上与未受累手和健康对照组的 S1 代表相似。我们没有发现受累手与未受累手的映射测量值与临床测量值(疼痛严重程度、上肢残疾、疾病持续时间)之间的差异关系。因此,如果发生任何映射重组,它似乎与疼痛和疾病严重程度没有直接关系。这些发现迫使我们重新考虑 CRPS 的皮质机制以及旨在“恢复”躯体定位代表以治疗疼痛的干预措施的基本原理。这项研究表明,手指在体感皮层中的空间图在慢性复杂性区域疼痛综合征(CRPS)中基本保持完整。这些发现对恢复复杂性区域疼痛综合征患者躯体定位代表的治疗原理提出了挑战。