Wretborn Jens, Ekelund Ulf, Wilhelms Daniel B
Department of Emergency Medicine, Local Health Care Services in Central Östergötland, Linköping, Sweden.
Department of Clinical Sciences Lund, Emergency Medicine, Faculty of Medicine, Lund University, Lund, Sweden.
Front Public Health. 2019 Sep 12;7:267. doi: 10.3389/fpubh.2019.00267. eCollection 2019.
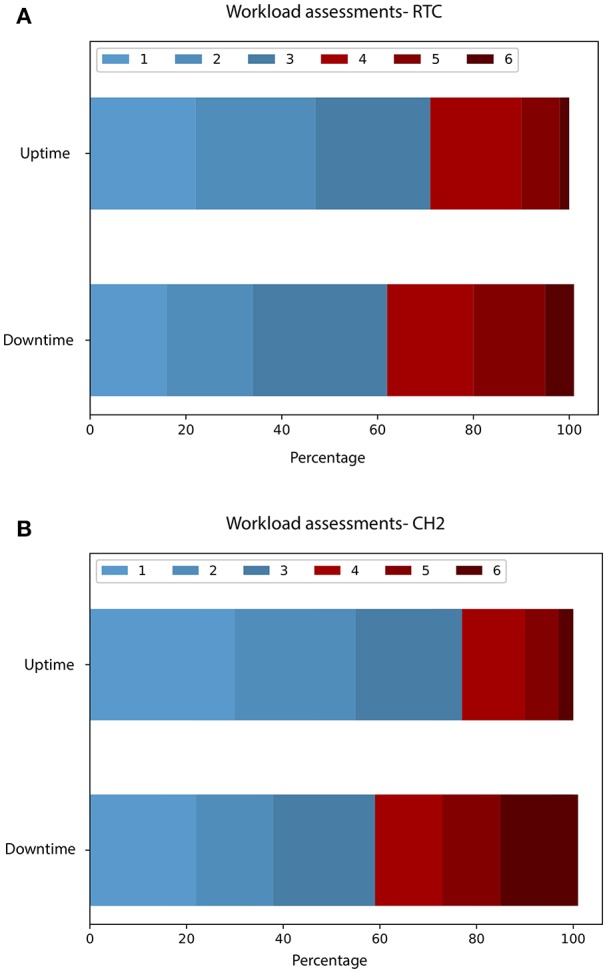
Emergency Departments (EDs) today rely heavily on Electronic Health Records (EHRs) and associated support systems. EHR updates are known to be associated with adverse events, but reports on the consequences of breakdowns in EDs are lacking. To describe the effects on workload, occupancy, patient Length Of Stay (LOS), and admissions at three EDs (a regional trauma center, a community hospital and a rural community hospital) during a 96 h period of EHR downtime, of which 48 h represented an unexpected breakdown. Assessments of workload, on a scale from 1 (no workload) to 6 (very high workload), were obtained from all staff before, during and after the downtime period. Occupancy, LOS and hospital admissions were extracted from data recorded in the fallback system at each ED during the downtime, and compared with the period before and after (uptime). Workload increased considerably at two EDs during the downtime whereas the third ED lacked resources to assess workload due to the breakdown. The proportion of assessments 4 were 28.5% during uptime compared to 38.4% during downtime at the regional trauma center ED (difference 9.9%, = 0.006, 95% CI 2.7-17%), and 22.9% compared to 41% at the rural community ED (difference 18.1%, = 0.0002, 95%CI 7.9-28.3%). Median LOS increased by 19 min (3:56 vs. 4:15, < 0.004) at the regional trauma center ED, by 76 min (3:34 vs. 4:50, < 0.001) at the community ED and was unaltered at the rural community ED (2:47 vs. 2:51, = 0.3) during downtime. Occupancy increased significantly at the community ED (1.59 vs. 0.71, < 0.0001). Admissions rates remained unchanged during the breakdown. Fallback systems and initiatives to manage the effects of the breakdown differed between the EDs. EHR downtime or unexpected breakdowns increased staff workload, and had variable effects on ED crowding as measured by LOS and occupancy. Additional staff and digital fallback systems may reduce the effects on ED crowding, but this descriptive study cannot determine causality.
如今,急诊科严重依赖电子健康记录(EHR)及相关支持系统。已知电子健康记录更新与不良事件相关,但缺乏关于急诊科系统故障后果的报告。本研究旨在描述在电子健康记录停机96小时期间(其中48小时为意外故障),三家急诊科(一家区域创伤中心、一家社区医院和一家农村社区医院)的工作量、床位占用率、患者住院时长及入院情况受到的影响。在停机前、停机期间和停机后,从所有工作人员处获取了工作量评估结果,评估范围为1(无工作量)至6(工作量极高)。停机期间,从各急诊科备用系统记录的数据中提取床位占用率、住院时长和医院入院情况,并与停机前后(正常运行)的时间段进行比较。在停机期间,两家急诊科的工作量大幅增加,而第三家急诊科因故障缺乏评估工作量的资源。在区域创伤中心急诊科,正常运行期间工作量评估为4级的比例为28.5%,停机期间为38.4%(差值9.9%,P = 0.006,95%置信区间2.7 - 17%);在农村社区急诊科,正常运行期间为22.9%,停机期间为41%(差值18.1%,P = 0.0002,95%置信区间7.9 - 28.3%)。在区域创伤中心急诊科,停机期间住院时长中位数增加了19分钟(3:56对比4:15,P < 0.004);在社区急诊科增加了76分钟(3:34对比4:50,P < 0.001);在农村社区急诊科未改变(2:47对比2:51,P = 0.3)。在社区急诊科,床位占用率显著增加(1.59对比0.71,P < 0.0001)。入院率在故障期间保持不变。各急诊科在备用系统及应对故障影响的举措方面存在差异。电子健康记录停机或意外故障增加了工作人员工作量,并对以住院时长和床位占用率衡量的急诊科拥挤情况产生了不同影响。额外的工作人员和数字备用系统可能会减少对急诊科拥挤情况的影响,但这项描述性研究无法确定因果关系。