Henry D. Janowitz Division of Gastroenterology, Department of Medicine, Icahn School of Medicine at Mount Sinai, New York, USA.
Department of Surgery, Icahn School of Medicine at Mount Sinai, New York, USA.
Aliment Pharmacol Ther. 2019 Dec;50(11-12):1189-1194. doi: 10.1111/apt.15505. Epub 2019 Oct 3.
The significance of endoscopic activity in asymptomatic ulcerative colitis (UC) patients with an ileal pouch is unknown.
To investigate the association of endoscopic pouch activity in asymptomatic patients with the subsequent development of pouchitis.
We analyzed a retrospective cohort of patients with UC or IBD-unspecified who underwent a total proctocolectomy with ileal pouch anal anastomosis (IPAA). Asymptomatic patients with a Pouchitis Disease Activity Index (PDAI) symptom sub-score of zero who underwent an index surveillance pouchoscopy were included. Endoscopic pouch body activity was graded as 0: normal, 1: mucosal inflammation, or 2: mucosal breaks (ulcers and/or erosions). The primary outcome was primary acute idiopathic pouchitis defined as PDAI score ≥ 7 with symptoms lasting less than four weeks and responsive to standard antibiotics, not otherwise meeting criteria for secondary pouchitis. The secondary outcome was chronic idiopathic pouchitis defined as PDAI score ≥ 7 with symptoms lasting greater than four weeks despite standard antibiotics. Predictors of pouchitis were analyzed using Kaplan-Meier and Cox regression methods with hazard ratios (HR) and 95% confidence intervals (CI) reported.
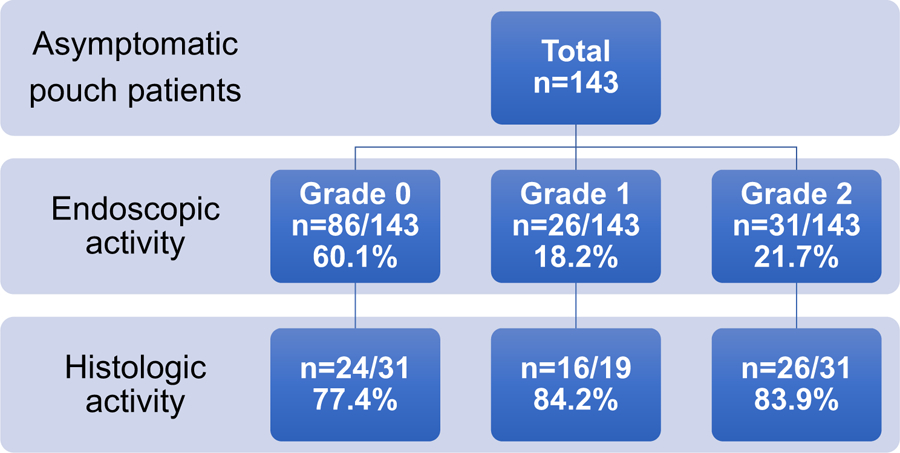
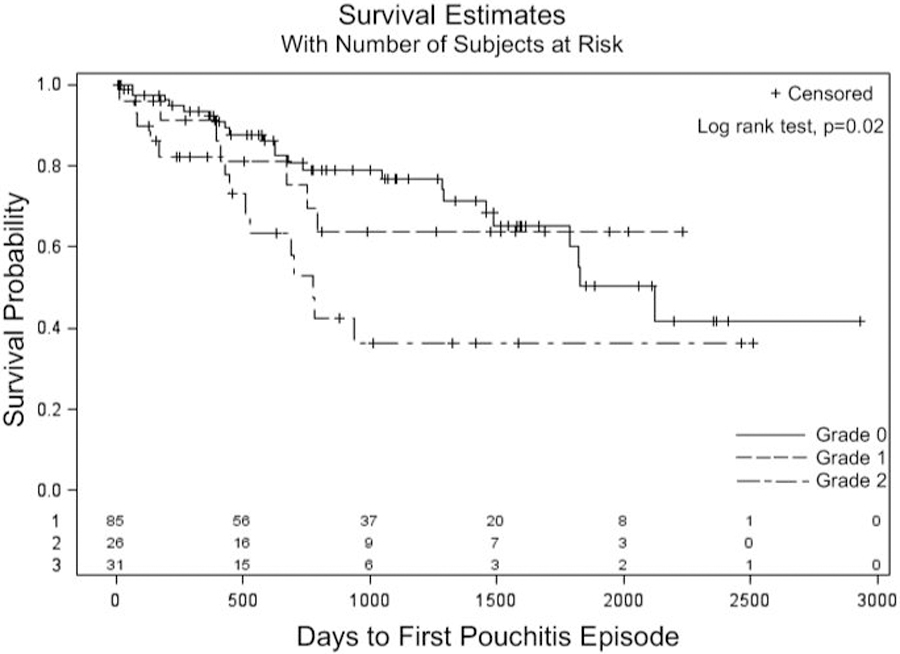
143 asymptomatic pouch patients were included. Index endoscopic pouch body activity was 0 in 86 (60.1%) patients, 1 in 26 (18.2%) and 2 in 31 (21.7%). The median length of follow-up after index surveillance pouchoscopy was 3.03 [IQR 1.24-4.60] years. Primary acute idiopathic pouchitis occurred in 44 (31%) patients and chronic idiopathic pouchitis in 12 (8.4%). Grade 2 endoscopic pouch activity was associated with the development of acute pouchitis (HR 2.39, 95% CI 1.23-4.67), although not chronic pouchitis (HR 1.76, 95% CI 0.53-5.87). Histologic inflammation in endoscopically normal pouch mucosa was not associated with acute or chronic pouchitis.
Mucosal breaks are present in nearly a quarter of asymptomatic patients with IPAA and are associated with an increased risk of acute pouchitis.
无症状溃疡性结肠炎(UC)患者行回肠储袋术后内镜下活动的意义尚不清楚。
探讨无症状患者内镜下储袋活动与随后发生储袋炎的关系。
我们分析了一组接受全直肠结肠切除加回肠储袋肛门吻合术(IPAA)的 UC 或未特指的 IBD 患者的回顾性队列。纳入接受指数监测储袋内镜检查且 Pouchitis 疾病活动指数(PDAI)症状亚评分(0 分)为无症状的患者。内镜下储袋体活动分级为 0:正常,1:黏膜炎症,或 2:黏膜破裂(溃疡和/或糜烂)。主要结局是原发性急性特发性储袋炎,定义为 PDAI 评分≥7,伴有持续少于 4 周的症状,对标准抗生素有反应,不符合继发性储袋炎标准。次要结局是慢性特发性储袋炎,定义为 PDAI 评分≥7,伴有持续超过 4 周的症状,尽管使用了标准抗生素。采用 Kaplan-Meier 和 Cox 回归方法分析储袋炎的预测因素,并报告风险比(HR)和 95%置信区间(CI)。
纳入 143 例无症状储袋患者。指数内镜下储袋体活动为 0 者 86 例(60.1%),1 者 26 例(18.2%),2 者 31 例(21.7%)。指数监测储袋内镜检查后中位随访时间为 3.03 年(IQR 1.24-4.60)。原发性急性特发性储袋炎发生于 44 例(31%)患者,慢性特发性储袋炎发生于 12 例(8.4%)。内镜下 2 级储袋活动与急性储袋炎的发生相关(HR 2.39,95%CI 1.23-4.67),但与慢性储袋炎无关(HR 1.76,95%CI 0.53-5.87)。内镜下正常储袋黏膜的组织学炎症与急性或慢性储袋炎无关。
IPAA 无症状患者中近四分之一存在黏膜破裂,与急性储袋炎风险增加相关。