School of Biomedical Engineering and Imaging Sciences, King's College, London, Fourth Floor Lambeth Wing, St Thomas' Hospital, London, SE1 7EH, UK.
Siemens Healthcare Limited, Frimley, UK.
J Cardiovasc Magn Reson. 2019 Oct 10;21(1):62. doi: 10.1186/s12968-019-0574-z.
Ex-vivo cardiovascular magnetic resonance (CMR) imaging has played an important role in the validation of in-vivo CMR characterization of pathological processes. However, comparison between in-vivo and ex-vivo imaging remains challenging due to shape changes occurring between the two states, which may be non-uniform across the diseased heart. A novel two-step process to facilitate registration between ex-vivo and in-vivo CMR was developed and evaluated in a porcine model of chronic myocardial infarction (MI).
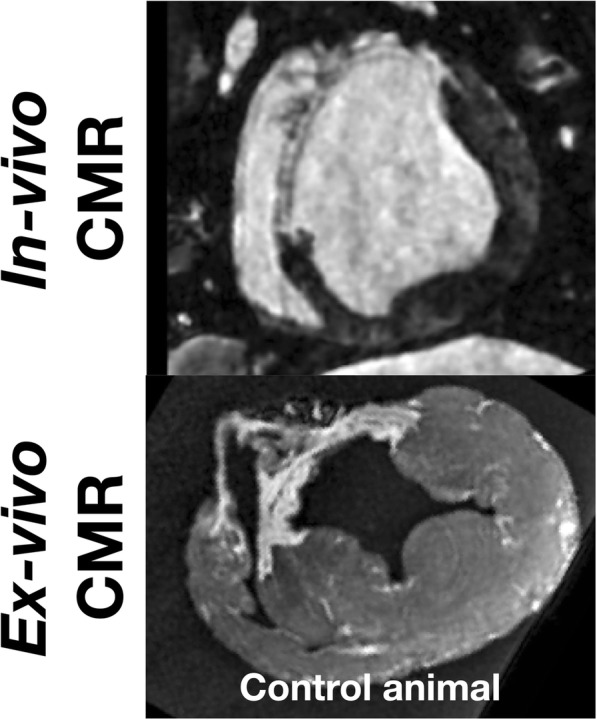
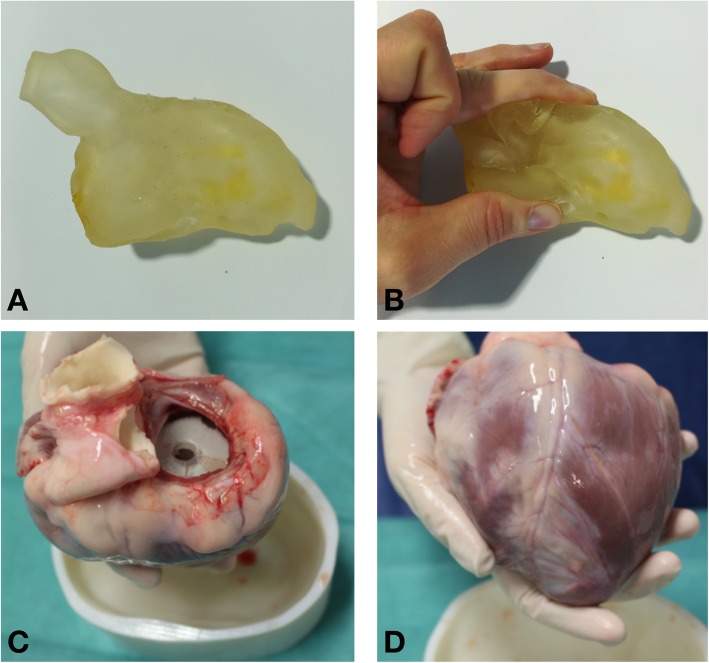
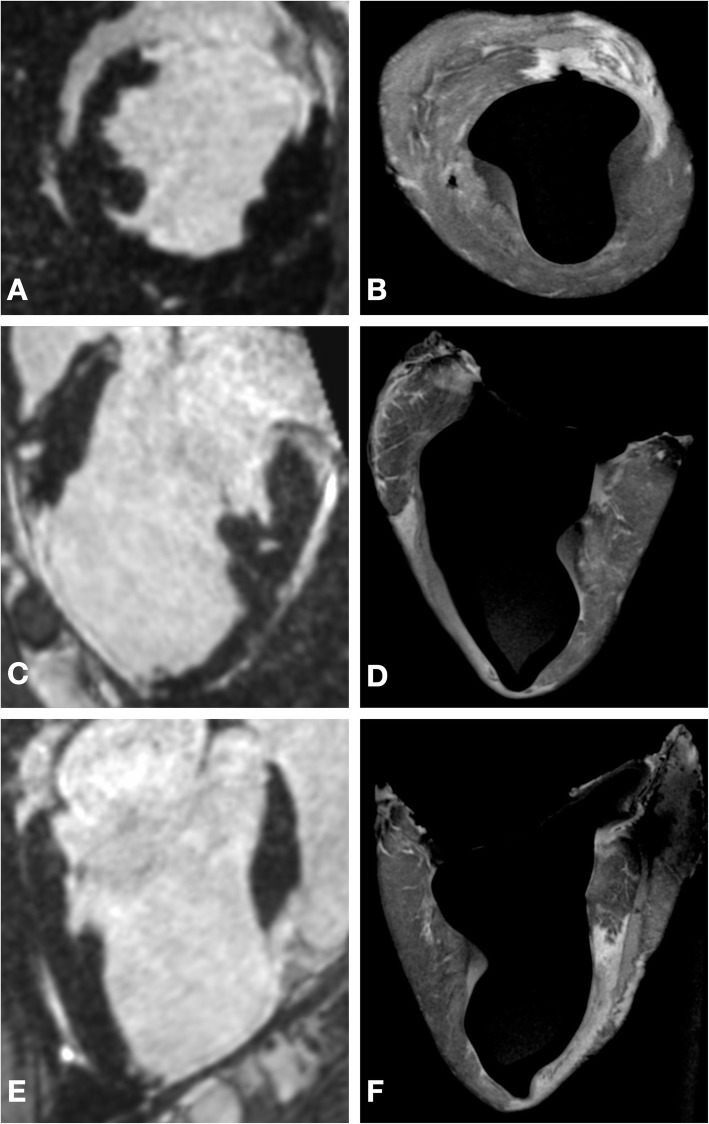
Seven weeks after ischemia-reperfusion MI, 12 swine underwent in-vivo CMR imaging with late gadolinium enhancement followed by ex-vivo CMR 1 week later. Five animals comprised the control group, in which ex-vivo imaging was undertaken without any support in the LV cavity, 7 animals comprised the experimental group, in which a two-step registration optimization process was undertaken. The first step involved a heart specific flexible 3D printed scaffold generated from in-vivo CMR, which was used to maintain left ventricular (LV) shape during ex-vivo imaging. In the second step, a non-rigid co-registration algorithm was applied to align in-vivo and ex-vivo data. Tissue dimension changes between in-vivo and ex-vivo imaging were compared between the experimental and control group. In the experimental group, tissue compartment volumes and thickness were compared between in-vivo and ex-vivo data before and after non-rigid registration. The effectiveness of the alignment was assessed quantitatively using the DICE similarity coefficient.
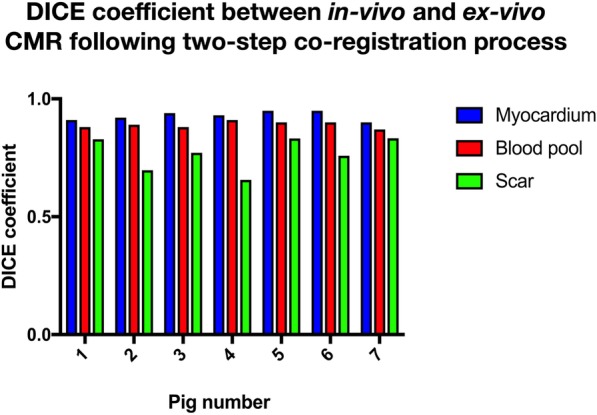
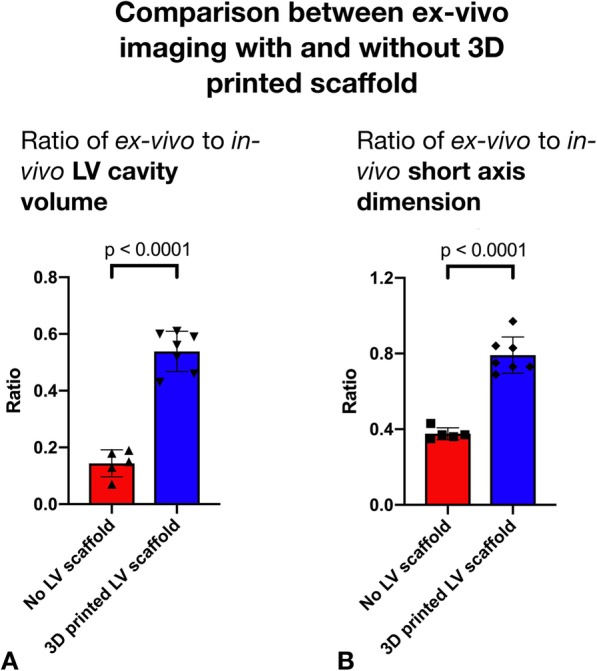
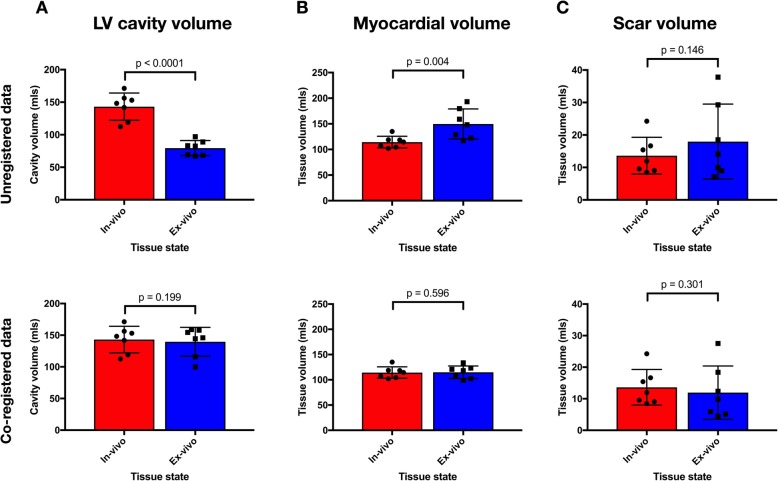
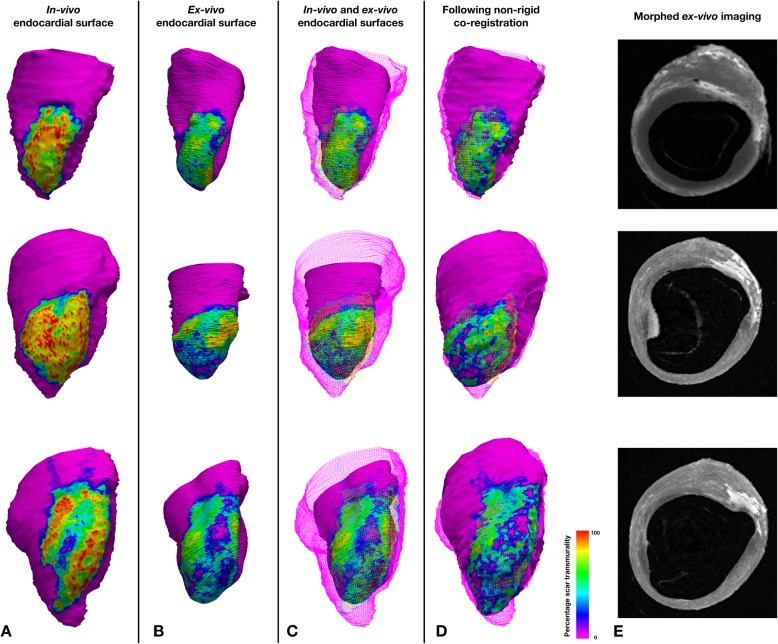
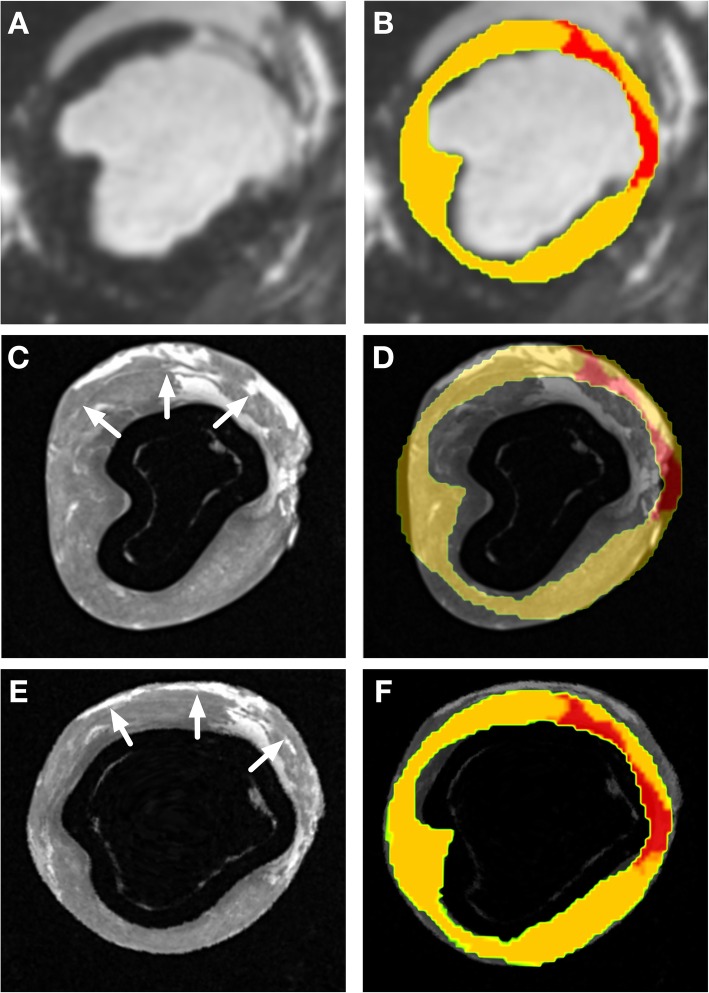
LV cavity volume changed more in the control group (ratio of cavity volume between ex-vivo and in-vivo imaging in control and experimental group 0.14 vs 0.56, p < 0.0001) and there was a significantly greater change in the short axis dimensions in the control group (ratio of short axis dimensions in control and experimental group 0.38 vs 0.79, p < 0.001). In the experimental group, prior to non-rigid co-registration the LV cavity contracted isotropically in the ex-vivo condition by less than 20% in each dimension. There was a significant proportional change in tissue thickness in the healthy myocardium (change = 29 ± 21%), but not in dense scar (change = - 2 ± 2%, p = 0.034). Following the non-rigid co-registration step of the process, the DICE similarity coefficients for the myocardium, LV cavity and scar were 0.93 (±0.02), 0.89 (±0.01) and 0.77 (±0.07) respectively and the myocardial tissue and LV cavity volumes had a ratio of 1.03 and 1.00 respectively.
The pattern of the morphological changes seen between the in-vivo and the ex-vivo LV differs between scar and healthy myocardium. A 3D printed flexible scaffold based on the in-vivo shape of the LV cavity is an effective strategy to minimize morphological changes in the ex-vivo LV. The subsequent non-rigid registration step further improved the co-registration and local comparison between in-vivo and ex-vivo data.
在活体心脏磁共振(CMR)特征描述的验证中,离体心血管磁共振成像发挥了重要作用。然而,由于在两个状态之间发生的形状变化,活体和离体成像之间的比较仍然具有挑战性,这种变化在患病心脏中可能不是均匀的。本研究提出并评估了一种新的两步法,以促进慢性心肌梗死(MI)猪模型的离体和活体 CMR 之间的配准。
在缺血再灌注 MI 后 7 周,12 只猪接受了晚期钆增强的活体 CMR 成像,1 周后进行了离体 CMR 成像。对照组中,5 只动物未在 LV 腔中进行任何支撑的情况下进行离体成像,实验组中,7 只动物进行了两步优化配准。第一步是使用活体 CMR 生成特定于心脏的柔性 3D 打印支架,以在离体成像过程中保持 LV 形状。在第二步中,应用非刚性配准算法来对齐活体和离体数据。比较实验组和对照组之间活体和离体成像之间的组织尺寸变化。在实验组中,比较了非刚性配准前后活体和离体数据的组织容积和厚度。使用 DICE 相似性系数定量评估对齐效果。
LV 腔体积在对照组中变化更大(对照组和实验组的腔体积比为 0.14 比 0.56,p<0.0001),对照组的短轴尺寸变化更大(对照组和实验组的短轴尺寸比为 0.38 比 0.79,p<0.001)。在实验组中,在非刚性配准之前,每个维度的 LV 腔在离体条件下的收缩幅度都不到 20%。健康心肌组织的厚度有明显的比例变化(变化为 29±21%),但致密瘢痕组织没有(变化为-2±2%,p=0.034)。在该过程的非刚性配准步骤之后,心肌、LV 腔和瘢痕的 DICE 相似系数分别为 0.93(±0.02)、0.89(±0.01)和 0.77(±0.07),心肌组织和 LV 腔体积的比例分别为 1.03 和 1.00。
活体和离体 LV 之间的形态变化模式在瘢痕和健康心肌组织之间有所不同。基于 LV 腔的体内形状的 3D 打印柔性支架是最小化离体 LV 形态变化的有效策略。随后的非刚性配准步骤进一步改善了活体和离体数据之间的配准和局部比较。