Nag Hirdaya Hulas, Sachan Ashish, Nekarakanti Phani Kumar
Department of GI Surgery, G B Pant Institute of Postgraduate Medical Education and Research, New Delhi, India.
J Minim Access Surg. 2021 Jan-Mar;17(1):21-27. doi: 10.4103/jmas.JMAS_98_19.
The outcome of laparoscopic extended cholecystectomy (EC) with wedge hepatic resection (LECW) in patients with gallbladder cancer (GBC) has been compared with that of open EC with wedge hepatic resection (OECW), but studies comparing laparoscopic EC with bi-segmentectomy (LECB) with open EC with bi-segmentectomy (OECB) are lacking.
This retrospective study comprised of 68 patients with GBC who were offered either LECB or OECB from July 2011 to July 2018. Patients were divided into laparoscopic group (LG) and open group (OG), and appropriate statistical methods were used for comparison.
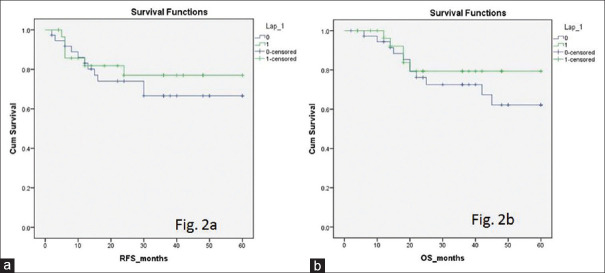
Out of the total 68 patients, 30 patients were in LG and 38 patients were in OG. Demographic, clinical and biochemical characteristics were similar except significantly higher number of male patients in OG (P = 0.01). In LG versus OG, the mean operation time was 286 versus 274 min (P = 0.565), mean blood loss was 158 versus 219 ml (P = 0.006) and mean hospital stay was 6.4 versus 9 days (P = 0.0001). The complication rate was 16.6% in LG and 31.5% in OG, but this difference was not statistically significant (P = 0.259). The median number of lymph nodes was 12 in both LG and OG (P = 0.62). Distribution of patients among American Joint Committee on Cancer stages I to IV was similar in both the groups (P = 0.5). Fifty percent of the patients in both the groups received adjuvant treatment (P = 1). In LG versus OG, the recurrence rate was 20% versus 28.9% (P = 0.4), mean recurrence-free survival was 48 months versus 44 months (P = 0.35) and overall survival was 51 months versus 46 months (P = 0.45). In LG versus OG, 1, 3 and 5-year survival was 96% versus 94%, 79% versus 72% and 79% versus 62% (P = 0.45). The median follow-up was statistically significantly shorter (24 vs. 36 months) in LG versus OG (P = 0.0001).
The oncological outcome and survival after LECB in patients with resectable GBC is not inferior to that after OECB. Laparoscopic approach has a potential to improve perioperative outcome in patients with GBC.
已将腹腔镜扩大胆囊切除术(EC)联合楔形肝切除术(LECW)治疗胆囊癌(GBC)患者的结果与开腹EC联合楔形肝切除术(OECW)的结果进行了比较,但缺乏比较腹腔镜EC联合肝段切除术(LECB)与开腹EC联合肝段切除术(OECB)的研究。
这项回顾性研究纳入了2011年7月至2018年7月期间接受LECB或OECB治疗的68例GBC患者。患者分为腹腔镜组(LG)和开腹组(OG),并采用适当的统计方法进行比较。
68例患者中,LG组30例,OG组38例。除OG组男性患者数量显著更多外(P = 0.01),两组的人口统计学、临床和生化特征相似。与OG组相比,LG组的平均手术时间为286分钟对274分钟(P = 0.565),平均失血量为158毫升对219毫升(P = 0.006),平均住院时间为6.4天对9天(P = 0.0001)。LG组的并发症发生率为16.6%,OG组为31.5%,但差异无统计学意义(P = 0.259)。LG组和OG组的中位淋巴结数量均为12个(P = 0.62)。两组患者在美国癌症联合委员会I至IV期的分布相似(P = 0.5)。两组中50%的患者接受了辅助治疗(P = 1)。与OG组相比,LG组的复发率为20%对28.9%(P = 0.4),平均无复发生存期为48个月对44个月(P = 0.35),总生存期为51个月对46个月(P = 0.45)。与OG组相比,LG组的1年、3年和5年生存率分别为96%对94%、79%对72%和79%对62%(P = 0.45)。LG组的中位随访时间在统计学上显著短于OG组(24个月对36个月)(P = 0.0001)。
可切除GBC患者接受LECB后的肿瘤学结局和生存率不低于OECB后的结果。腹腔镜手术方法有可能改善GBC患者的围手术期结局。