Paulsen Michael J, Imbrie-Moore Annabel M, Wang Hanjay, Bae Jung Hwa, Hironaka Camille E, Farry Justin M, Lucian Haley J, Thakore Akshara D, MacArthur John W, Cutkosky Mark R, Woo Y Joseph
Department of Cardiothoracic Surgery, Stanford University, Stanford, CA, USA.
Department of Mechanical Engineering, Stanford University, Stanford, CA, USA.
Eur J Cardiothorac Surg. 2020 Mar 1;57(3):535-544. doi: 10.1093/ejcts/ezz258.
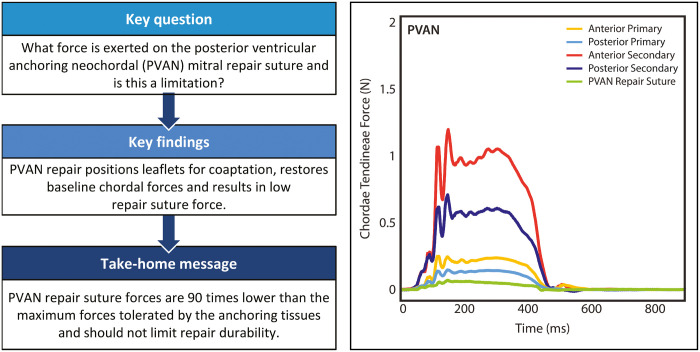
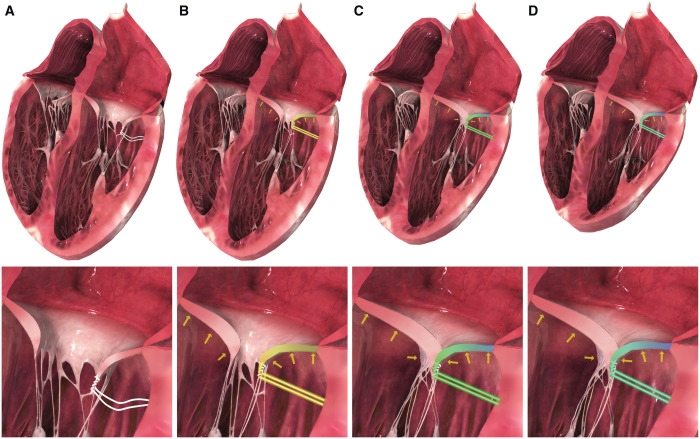
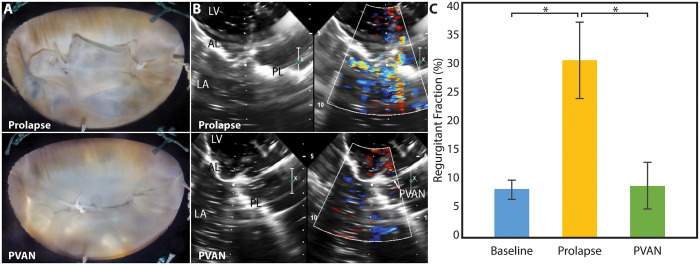
Posterior ventricular anchoring neochordal (PVAN) repair is a non-resectional technique for correcting mitral regurgitation (MR) due to posterior leaflet prolapse, utilizing a single suture anchored in the myocardium behind the leaflet. This technique has demonstrated clinical efficacy, although a theoretical limitation is stability of the anchoring suture. We hypothesize that the PVAN suture positions the leaflet for coaptation, after which forces are distributed evenly with low repair suture forces.
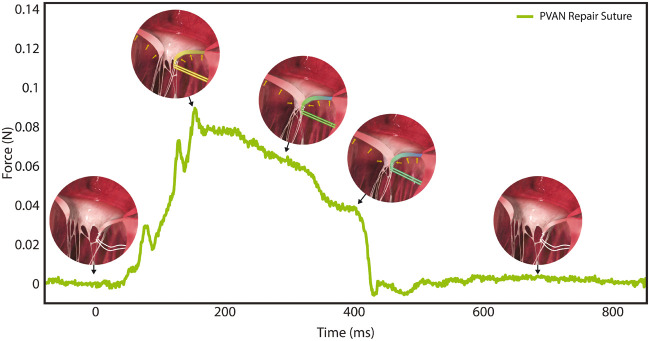
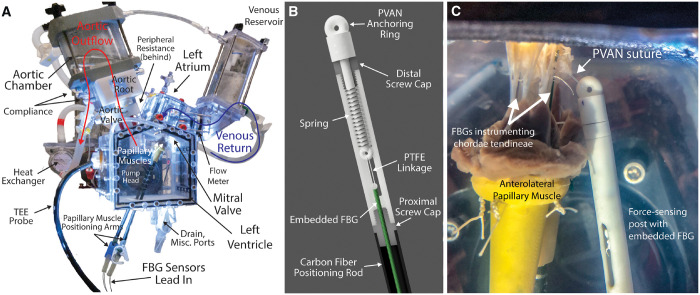
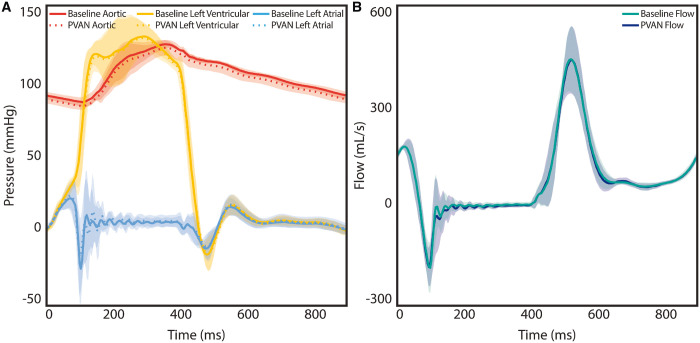
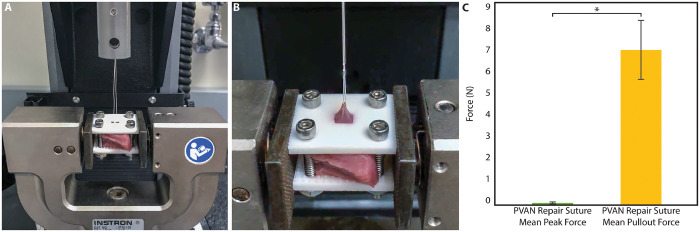
Porcine mitral valves were mounted in a 3-dimensional-printed heart simulator and chordal forces, haemodynamics and echocardiography were collected at baseline, after inducing MR by severing chordae, and after PVAN repair. Repair suture forces were measured with a force-sensing post positioned to mimic in vivo suture placement. Forces required to pull the myocardial suture free were also determined.
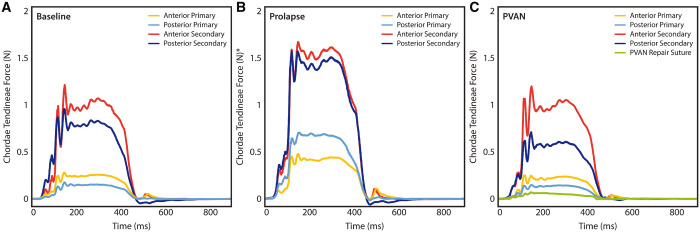
Relative primary and secondary chordae forces on both leaflets were elevated during prolapse (P < 0.05). PVAN repair eliminated MR in all valves and normalized chordae forces to baseline levels on anterior primary (0.37 ± 0.23 to 0.22 ± 0.09 N, P < 0.05), posterior primary (0.62 ± 0.37 to 0.14 ± 0.05 N, P = 0.001), anterior secondary (1.48 ± 0.52 to 0.85 ± 0.43 N, P < 0.001) and posterior secondary chordae (1.42 ± 0.69 to 0.59 ± 0.17 N, P = 0.005). Repair suture forces were minimal, even compared to normal primary chordae forces (0.08 ± 0.04 vs 0.19 ± 0.08 N, P = 0.002), and were 90 times smaller than maximum forces tolerated by the myocardium (0.08 ± 0.04 vs 6.9 ± 1.3 N, P < 0.001).
PVAN repair eliminates MR by positioning the posterior leaflet for coaptation, distributing forces throughout the valve. Given extremely low measured forces, the strength of the repair suture and the myocardium is not a limitation.
后心室锚定新腱索(PVAN)修复术是一种用于纠正因后叶脱垂导致的二尖瓣反流(MR)的非切除技术,该技术利用一根缝合线锚定在瓣叶后方的心肌中。尽管该技术存在锚定缝合线稳定性这一理论局限性,但已证明其具有临床疗效。我们假设PVAN缝合线将瓣叶定位以实现对合,在此之后力会以较低的修复缝合线力均匀分布。
将猪二尖瓣安装在三维打印的心脏模拟器中,在基线时、切断腱索诱导二尖瓣反流后以及PVAN修复后收集腱索力、血流动力学和超声心动图数据。使用一个力敏柱测量修复缝合线力,该力敏柱的位置模拟体内缝合线放置。还确定了将心肌缝合线拉出所需的力。
在脱垂期间,两个瓣叶上的相对原发性和继发性腱索力均升高(P < 0.05)。PVAN修复消除了所有瓣膜的二尖瓣反流,并使原发性前叶(从0.37±0.23 N至0.22±0.09 N,P < 0.05)、原发性后叶(从0.62±0.37 N至0.14±0.05 N,P = 0.001)、继发性前叶(从1.48±0.52 N至0.85±0.43 N,P < 0.001)和继发性后叶腱索(从1.42±0.69 N至0.59±0.17 N,P = 0.005)的腱索力恢复到基线水平。修复缝合线力极小,甚至与正常原发性腱索力相比也是如此(0.08±0.04 N对0.19±0.08 N,P = 0.002),并且比心肌所能耐受的最大力小90倍(0.08±0.04 N对6.9±1.3 N,P < 0.001)。
PVAN修复通过将后叶定位以实现对合,使力在整个瓣膜上分布,从而消除二尖瓣反流。鉴于所测量的力极低,修复缝合线和心肌的强度不是一个限制因素。