Wentzel Nicole, Panieri Angelica, Ayazi Maryam, Ntshalintshali Sipho Duncan, Pourpak Zahra, Hawarden Di, Potter Paul, Levin Michael E, Fazlollahi Mohammad Reza, Peter Jonathan
Faculty of Health Sciences, University of Cape Town, South Africa.
Immunology, Asthma and Allergy Research Institute, Tehran University of Medical Sciences, Tehran, Iran.
World Allergy Organ J. 2019 Oct 12;12(9):100049. doi: 10.1016/j.waojou.2019.100049. eCollection 2019 Sep.
International guideline-recommended on-demand treatments for hereditary angioedema (HAE) include: C1-esterase inhibitor (plasma-derived or recombinant), or bradykinin-receptor antagonists. In most low- and middle-income countries (LMIC) these products are not registered or are unaffordable. Solvent-detergent, fresh or freeze-dried plasma therapy is thus the only available on-demand treatment in these settings; but published data on efficacy and safety are limited. This study evaluated the efficacy and safety of on-demand plasma treatment of acute HAE in two LMICs.
A retrospective folder or patient registry review of acute swelling episodes necessitating emergency room attendance amongst known HAE patients was conducted at treatment centers in South Africa and Iran. Data collected included the site of angioedema, timing and amount of fresh frozen plasma (FFP) administered, time-to-resolution, hospital length of stay and adverse events.
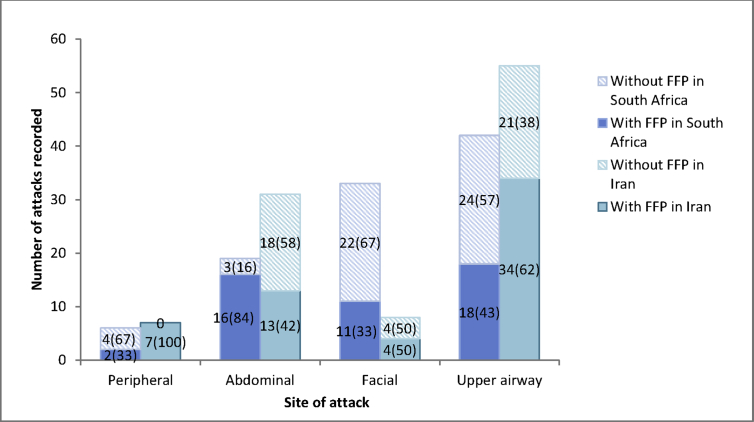
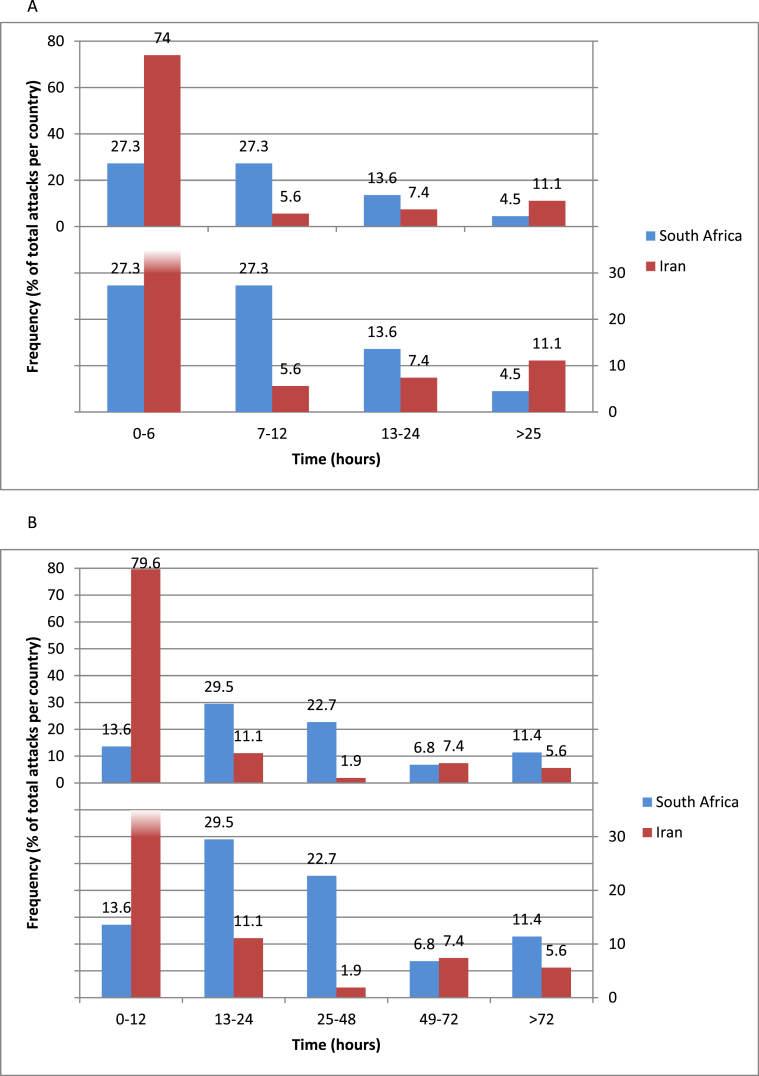
There were 176 acute swelling episodes amongst 43 HAE patients; 98 were treated with FFP. The face, upper airway, and abdomen were involved in 15.3% (15/98), 53.1% (52/98) and 29.6% (29/98) of episodes treated with FFP respectively. Median (interquartile range ([IQR]) of FFP administered was 400 (280-560) mLs. In all episodes except two, FFP led to resolution, with median (IQR) hours to resolution 4 (2-12). Five transfusion reactions occurred, with one case of anaphylaxis and no deaths; giving an adverse reaction rate of 5%. Differences between South Africa and Iran included: (1) proportion of HAE type II(2) median (IQR) hours to FFP administration and hospitalization, (3) number of intubations after FFP infusion. Healthcare cost for FFP treatment was USD369- 791 in South Africa and USD275-550 in Iran, largely influenced by hospital length of stay.
Plasma (fresh-frozen) remains the only available effective on-demand treatment for acute HAE in many countries. FFP is effective and safe, but time-to-resolution is slower and adverse events are more frequent than published data on targeted therapies. Overall healthcare cost of FFP approaches that of targeted therapies - now available through global access programs - when hospitalization is prolonged.
国际指南推荐的遗传性血管性水肿(HAE)按需治疗方法包括:C1酯酶抑制剂(血浆源性或重组型)或缓激肽受体拮抗剂。在大多数低收入和中等收入国家(LMIC),这些产品未注册或价格昂贵。因此,溶剂去污、新鲜或冻干血浆疗法是这些地区唯一可用的按需治疗方法;但已发表的关于其疗效和安全性的数据有限。本研究评估了在两个低收入和中等收入国家对急性HAE进行按需血浆治疗的疗效和安全性。
在南非和伊朗的治疗中心,对已知HAE患者中需要急诊室就诊的急性肿胀发作进行回顾性病历或患者登记审查。收集的数据包括血管性水肿的部位、新鲜冰冻血浆(FFP)的给药时间和剂量、消退时间、住院时间和不良事件。
43例HAE患者中有176次急性肿胀发作;98例接受了FFP治疗。接受FFP治疗的发作中,面部、上呼吸道和腹部受累分别占15.3%(15/98)、53.1%(52/98)和29.6%(29/98)。FFP给药的中位数(四分位间距[IQR])为400(280 - 560)毫升。除两例发作外,所有发作FFP均导致症状消退,消退的中位数(IQR)时间为4(2 - 12)小时。发生了5例输血反应,1例过敏反应,无死亡病例;不良反应发生率为5%。南非和伊朗之间的差异包括:(1)II型HAE的比例;(2)FFP给药和住院的中位数(IQR)时间;(3)FFP输注后插管的次数。南非FFP治疗的医疗费用为369 - 791美元,伊朗为275 - 550美元,很大程度上受住院时间影响。
在许多国家,血浆(新鲜冰冻)仍然是急性HAE唯一可用的有效按需治疗方法。FFP有效且安全,但与已发表的靶向治疗数据相比,消退时间较慢,不良事件更频繁。当住院时间延长时,FFP的总体医疗费用接近靶向治疗(现在可通过全球获取计划获得)的费用。