Lancet Gastroenterol Hepatol. 2019 Dec;4(12):934-947. doi: 10.1016/S2468-1253(19)30347-4. Epub 2019 Oct 21.
Worldwide, both the incidence and death rates of pancreatic cancer are increasing. Evaluation of pancreatic cancer burden and its global, regional, and national patterns is crucial to policy making and better resource allocation for controlling pancreatic cancer risk factors, developing early detection methods, and providing faster and more effective treatments.
Vital registration, vital registration sample, and cancer registry data were used to generate mortality, incidence, and disability-adjusted life-years (DALYs) estimates. We used the comparative risk assessment framework to estimate the proportion of deaths attributable to risk factors for pancreatic cancer: smoking, high fasting plasma glucose, and high body-mass index. All of the estimates were reported as counts and age-standardised rates per 100 000 person-years. 95% uncertainty intervals (UIs) were reported for all estimates.
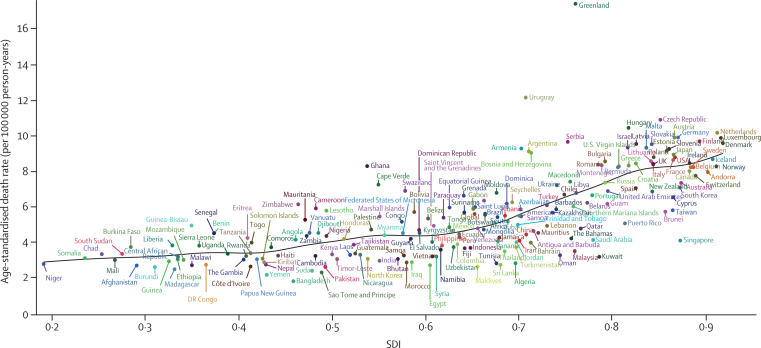
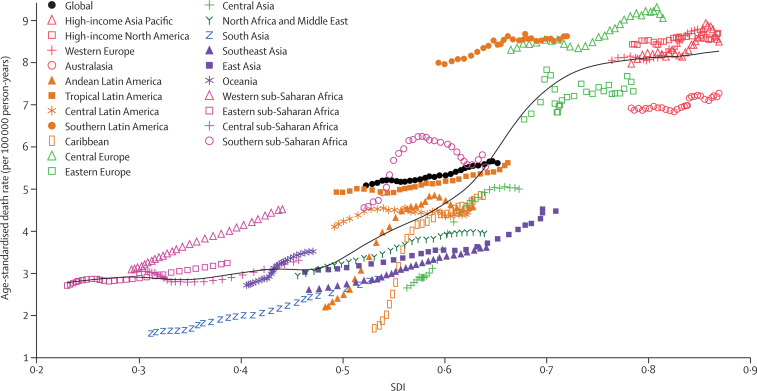
In 2017, there were 448 000 (95% UI 439 000-456 000) incident cases of pancreatic cancer globally, of which 232 000 (210 000-221 000; 51·9%) were in males. The age-standardised incidence rate was 5·0 (4·9-5·1) per 100 000 person-years in 1990 and increased to 5·7 (5·6-5·8) per 100 000 person-years in 2017. There was a 2·3 times increase in number of deaths for both sexes from 196 000 (193 000-200 000) in 1990 to 441 000 (433 000-449 000) in 2017. There was a 2·1 times increase in DALYs due to pancreatic cancer, increasing from 4·4 million (4·3-4·5) in 1990 to 9·1 million (8·9-9·3) in 2017. The age-standardised death rate of pancreatic cancer was highest in the high-income super-region across all years from 1990 to 2017. In 2017, the highest age-standardised death rates were observed in Greenland (17·4 [15·8-19·0] per 100 000 person-years) and Uruguay (12·1 [10·9-13·5] per 100 000 person-years). These countries also had the highest age-standardised death rates in 1990. Bangladesh (1·9 [1·5-2·3] per 100 000 person-years) had the lowest rate in 2017, and São Tomé and Príncipe (1·3 [1·1-1·5] per 100 000 person-years) had the lowest rate in 1990. The numbers of incident cases and deaths peaked at the ages of 65-69 years for males and at 75-79 years for females. Age-standardised pancreatic cancer deaths worldwide were primarily attributable to smoking (21·1% [18·8-23·7]), high fasting plasma glucose (8·9% [2·1-19·4]), and high body-mass index (6·2% [2·5-11·4]) in 2017.
Globally, the number of deaths, incident cases, and DALYs caused by pancreatic cancer has more than doubled from 1990 to 2017. The increase in incidence of pancreatic cancer is likely to continue as the population ages. Prevention strategies should focus on modifiable risk factors. Development of screening programmes for early detection and more effective treatment strategies for pancreatic cancer are needed.
Bill & Melinda Gates Foundation.

在全球范围内,胰腺癌的发病率和死亡率都在上升。评估胰腺癌的负担及其在全球、区域和国家的模式对于制定政策以及更好地分配资源以控制胰腺癌的危险因素、开发早期检测方法以及提供更快和更有效的治疗方法至关重要。
使用生命登记、生命登记抽样和癌症登记数据来生成死亡率、发病率和伤残调整生命年 (DALY) 的估计值。我们使用比较风险评估框架来估计归因于胰腺癌风险因素的死亡比例:吸烟、空腹血糖高和身体质量指数高。所有估计值均以每 10 万人年的计数和年龄标准化率报告。所有估计值均报告了 95%的置信区间 (UI)。
2017 年,全球有 44.8 万 (95% UI 43.9 万-45.6 万) 例胰腺癌新发病例,其中 23.2 万 (21.0 万-22.1 万;51.9%) 为男性。1990 年,年龄标准化发病率为每 10 万人年 5.0 (4.9-5.1),到 2017 年增加到 5.7 (5.6-5.8)。1990 年男女死亡人数为 19.6 万 (19.3 万-20 万),到 2017 年增加到 44.1 万 (43.3 万-44.9 万),增加了两倍多。2017 年因胰腺癌导致的 DALY 增加了两倍,从 1990 年的 440 万 (43.3-44.5)增加到 910 万 (8.9-9.3)。1990 年至 2017 年,高收入超级地区的胰腺癌年龄标准化死亡率一直最高。2017 年,格陵兰 (17.4 [15.8-19.0] 每 10 万人年) 和乌拉圭 (12.1 [10.9-13.5] 每 10 万人年) 的年龄标准化死亡率最高。这些国家在 1990 年的死亡率也最高。2017 年,孟加拉国的发病率最低 (1.9 [1.5-2.3] 每 10 万人年),圣多美和普林西比的发病率最低 (1.3 [1.1-1.5] 每 10 万人年),1990 年。男性胰腺癌发病和死亡人数的峰值出现在 65-69 岁,女性出现在 75-79 岁。2017 年,全球归因于吸烟 (21.1% [18.8-23.7])、空腹血糖高 (8.9% [2.1-19.4]) 和高身体质量指数 (6.2% [2.5-11.4]) 的胰腺癌死亡人数主要归因于吸烟。
全球范围内,1990 年至 2017 年间,胰腺癌的死亡人数、发病例数和 DALY 增加了一倍以上。随着人口老龄化,胰腺癌的发病率可能会继续上升。预防策略应侧重于可改变的危险因素。需要开发早期检测的筛查计划和更有效的胰腺癌治疗策略。
比尔及梅琳达·盖茨基金会。