Lancet Gastroenterol Hepatol. 2020 Jun;5(6):582-597. doi: 10.1016/S2468-1253(20)30007-8. Epub 2020 Apr 1.
Oesophageal cancer is a common and often fatal cancer that has two main histological subtypes: oesophageal squamous cell carcinoma and oesophageal adenocarcinoma. Updated statistics on the incidence and mortality of oesophageal cancer, and on the disability-adjusted life-years (DALYs) caused by the disease, can assist policy makers in allocating resources for prevention, treatment, and care of oesophageal cancer. We report the latest estimates of these statistics for 195 countries and territories between 1990 and 2017, by age, sex, and Socio-demographic Index (SDI), using data from the Global Burden of Diseases, Injuries, and Risk Factors Study 2017 (GBD).
We used data from vital registration systems, vital registration-samples, verbal autopsy records, and cancer registries, combined with relevant modelling, to estimate the mortality, incidence, and burden of oesophageal cancer from 1990 to 2017. Mortality-to-incidence ratios (MIRs) were estimated and fed into a Cause of Death Ensemble model (CODEm) including risk factors. MIRs were used for mortality and non-fatal modelling. Estimates of DALYs attributable to the main risk factors of oesophageal cancer available in GBD were also calculated. The proportion of oesophageal squamous cell carcinoma to all oesophageal cancers was extracted by use of publicly available data, and its variation was examined against SDI, the Healthcare Access and Quality (HAQ) Index, and available risk factors in GBD that are specific for oesophageal squamous cell carcinoma (eg, unimproved water source and indoor air pollution) and for oesophageal adenocarcinoma (gastro-oesophageal reflux disease).
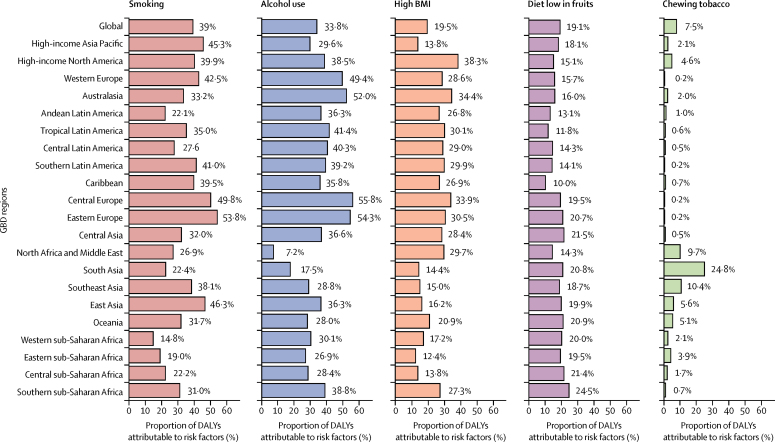
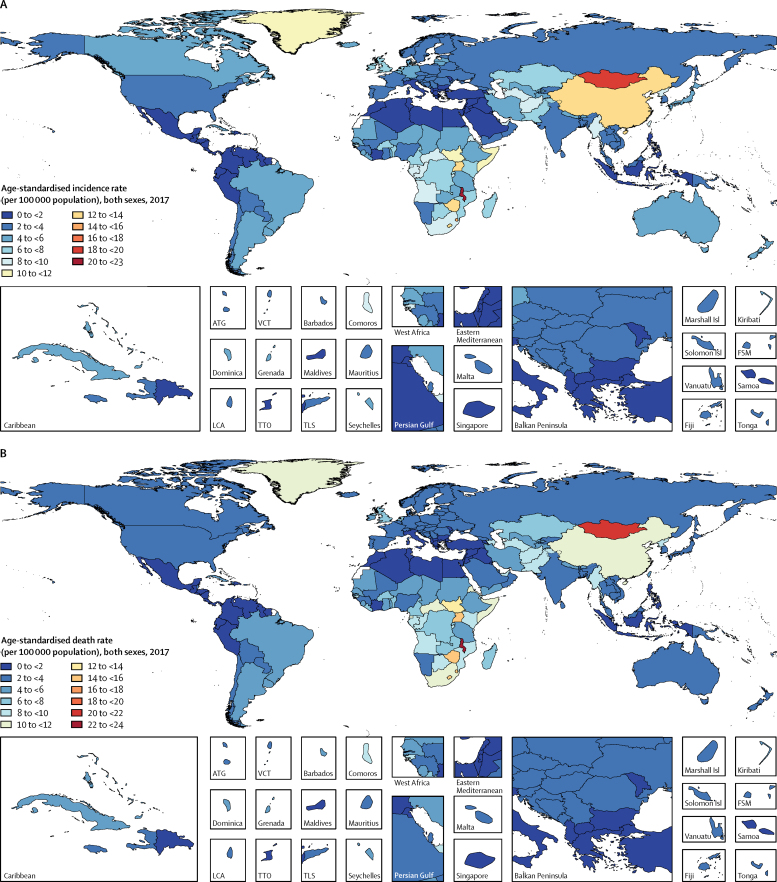
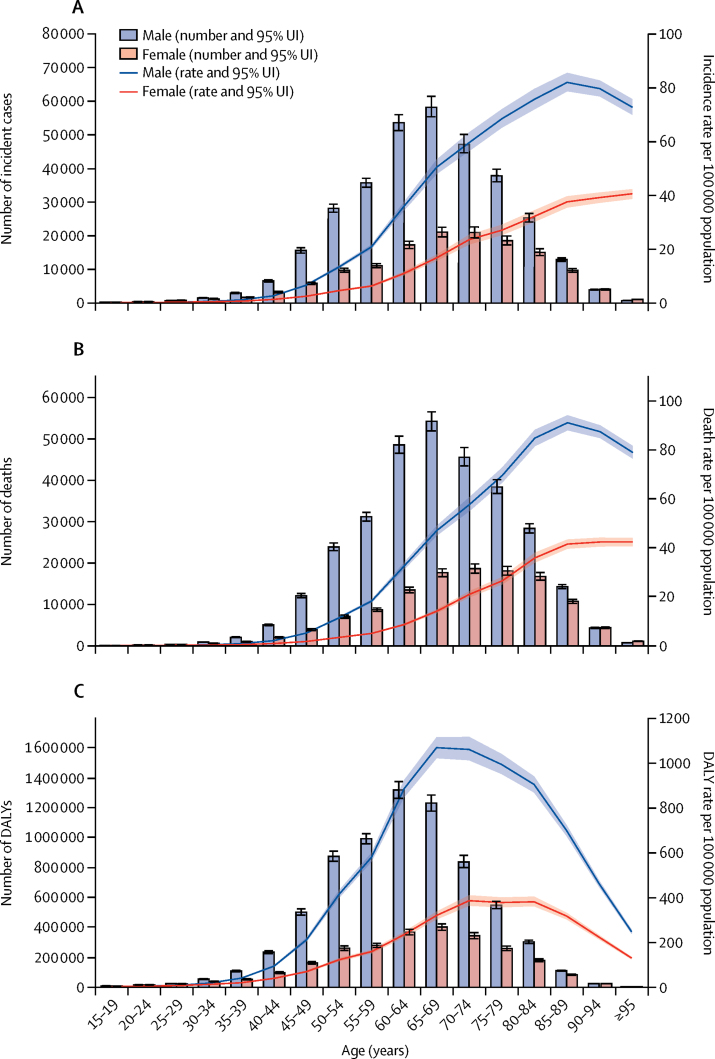
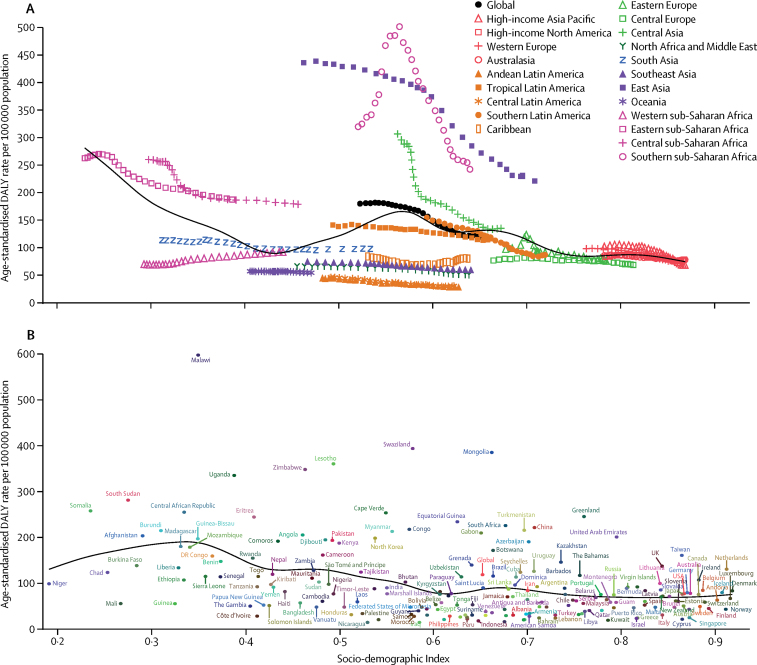
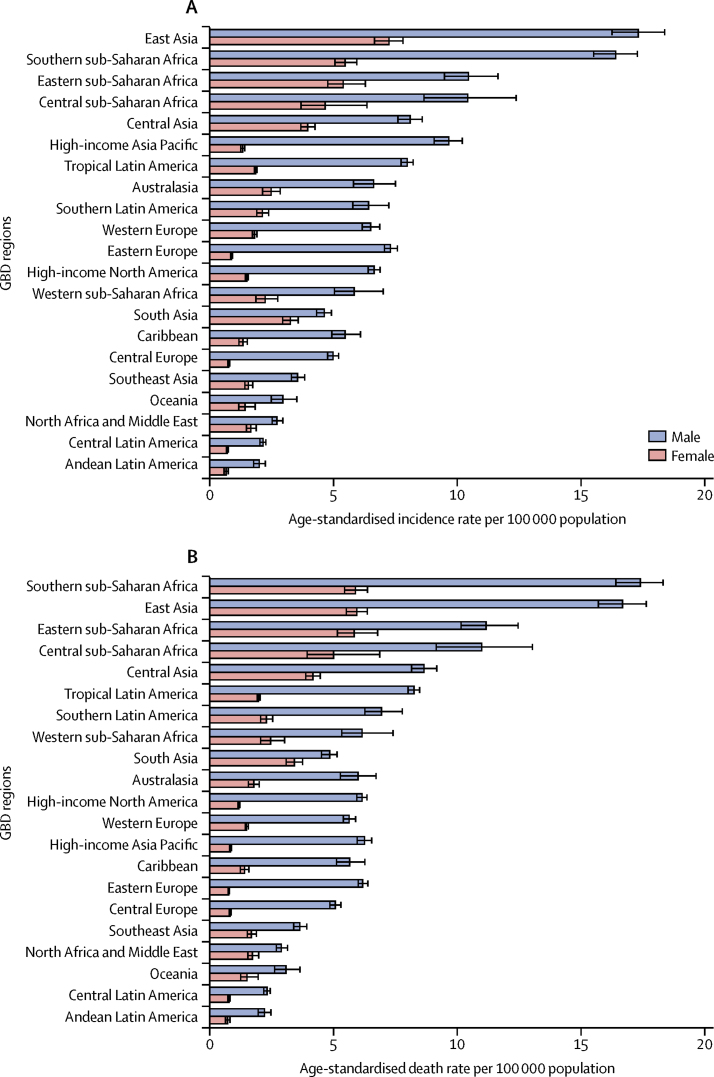
There were 473 000 (95% uncertainty interval [95% UI] 459 000-485 000) new cases of oesophageal cancer and 436 000 (425 000-448 000) deaths due to oesophageal cancer in 2017. Age-standardised incidence was 5·9 (5·7-6·1) per 100 000 population and age-standardised mortality was 5·5 (5·3-5·6) per 100 000. Oesophageal cancer caused 9·78 million (9·53-10·03) DALYs, with an age-standardised rate of 120 (117-123) per 100 000 population. Between 1990 and 2017, age-standardised incidence decreased by 22·0% (18·6-25·2), mortality decreased by 29·0% (25·8-32·0), and DALYs decreased by 33·4% (30·4-36·1) globally. However, as a result of population growth and ageing, the total number of new cases increased by 52·3% (45·9-58·9), from 310 000 (300 000-322 000) to 473 000 (459 000-485 000); the number of deaths increased by 40·0% (34·1-46·3), from 311 000 (301 000-323 000) to 436 000 (425 000-448 000); and total DALYs increased by 27·4% (22·1-33·1), from 7·68 million (7·42-7·97) to 9·78 million (9·53-10·03). At the national level, China had the highest number of incident cases (235 000 [223 000-246 000]), deaths (213 000 [203 000-223 000]), and DALYs (4·46 million [4·25-4·69]) in 2017. The highest national-level age-standardised incidence rates in 2017 were observed in Malawi (23·0 [19·4-26·5] per 100 000 population) and Mongolia (18·5 [16·4-20·8] per 100 000). In 2017, age-standardised incidence was 2·7 times higher, mortality 2·9 times higher, and DALYs 3·0 times higher in males than in females. In 2017, a substantial proportion of oesophageal cancer DALYs were attributable to known risk factors: tobacco smoking (39·0% [35·5-42·2]), alcohol consumption (33·8% [27·3-39·9]), high BMI (19·5% [6·3-36·0]), a diet low in fruits (19·1% [4·2-34·6]), and use of chewing tobacco (7·5% [5·2-9·6]). Countries with a low SDI and HAQ Index and high levels of indoor air pollution had a higher proportion of oesophageal squamous cell carcinoma to all oesophageal cancer cases than did countries with a high SDI and HAQ Index and with low levels of indoor air pollution.
Despite reductions in age-standardised incidence and mortality rates, oesophageal cancer remains a major cause of cancer mortality and burden across the world. Oesophageal cancer is a highly fatal disease, requiring increased primary prevention efforts and, possibly, screening in some high-risk areas. Substantial variation exists in age-standardised incidence rates across regions and countries, for reasons that are unclear.
Bill & Melinda Gates Foundation.
食管癌是一种常见且通常致命的癌症,具有两种主要的组织学亚型:食管鳞状细胞癌和食管腺癌。食管癌发病率和死亡率以及疾病导致的伤残调整生命年(DALYs)的最新统计数据可以帮助政策制定者为食管癌的预防、治疗和护理分配资源。我们报告了 195 个国家和地区 1990 年至 2017 年的最新发病率、死亡率和疾病负担估计值,按年龄、性别和社会人口指数(SDI)划分,并使用了 2017 年全球疾病、伤害和危险因素研究(GBD)的数据。
我们使用来自生命登记系统、生命登记抽样、死因推断记录和癌症登记处的数据,并结合相关模型,估算了 1990 年至 2017 年食管癌的死亡率、发病率和疾病负担。死亡率与发病率之比(MIRs)被估算出来,并被输入包括风险因素的死因综合模型(CODEm)。MIRs 被用于死亡率和非致死性模型。在 GBD 中也计算了食管癌主要风险因素导致的 DALYs 估计值。从公开获得的数据中提取了食管鳞状细胞癌与所有食管癌病例的比例,并对其与 SDI、医疗保健获取和质量(HAQ)指数以及 GBD 中特定于食管鳞状细胞癌(如未改善的水源和室内空气污染)和食管腺癌(胃食管反流病)的风险因素进行了比较。
2017 年,有 47.3 万(95%置信区间[95%CI]45.9 万-48.5 万)例新食管癌病例和 43.6 万(42.5 万-44.8 万)例食管癌死亡。年龄标准化发病率为 5.9(5.7-6.1)/10 万,年龄标准化死亡率为 5.5(5.3-5.6)/10 万。食管癌导致 978 万(953-1003)DALYs,年龄标准化率为 120(117-123)/10 万。1990 年至 2017 年,年龄标准化发病率下降了 22.0%(18.6-25.2),死亡率下降了 29.0%(25.8-32.0),全球 DALYs 下降了 33.4%(30.4-36.1)。然而,由于人口增长和老龄化,新发病例总数增加了 52.3%(45.9-58.9),从 31 万(30 万-32.2 万)增加到 47.3 万(45.9 万-48.5 万);死亡人数增加了 40.0%(34.1-46.3),从 31.1 万(30.1 万-32.3 万)增加到 43.6 万(42.5 万-44.8 万);总 DALYs 增加了 27.4%(22.1-33.1),从 768 万(742-797)增加到 978 万(953-1003)。在国家层面上,中国的发病例数(235 万[223 万-246 万])、死亡人数(213 万[203 万-223 万])和 DALYs(446 万[425-469 万])最高。2017 年,马拉维(23.0[19.4-26.5]/10 万)和蒙古(18.5[16.4-20.8])的全国发病率最高。2017 年,男性食管癌年龄标准化发病率是女性的 2.7 倍,死亡率是女性的 2.9 倍,DALYs 是女性的 3.0 倍。2017 年,食管癌的 DALYs 有很大一部分归因于已知的风险因素:吸烟(39.0%[35.5-42.2])、饮酒(33.8%[27.3-39.9])、高 BMI(19.5%[6.3-36.0])、水果摄入量低(19.1%[4.2-34.6])和咀嚼烟草使用(7.5%[5.2-9.6])。SDI 和 HAQ 指数低、室内空气污染水平高的国家与 SDI 和 HAQ 指数高、室内空气污染水平低的国家相比,食管鳞状细胞癌占所有食管癌病例的比例更高。
尽管年龄标准化发病率和死亡率有所下降,但食管癌仍然是全球癌症死亡和疾病负担的主要原因。食管癌是一种高度致命的疾病,需要加强初级预防工作,并可能在一些高危地区进行筛查。不同地区和国家之间的年龄标准化发病率存在很大差异,原因尚不清楚。
比尔及梅琳达·盖茨基金会。