MRC Integrative Epidemiology Unit Bristol Medical School University of Bristol Bristol UK; Epidemiology of Cancer and Healthcare Outcomes (ECHO) Group, Research Department of Behavioural Science and Health, University College London, 1-19 Torrington Place, London, UK.
National Cancer Registration and Analysis Service (NCRAS), Public Health England, 6th Floor, Wellington House, 135-155 Waterloo Road, London, UK.
Cancer Epidemiol. 2019 Dec;63:101574. doi: 10.1016/j.canep.2019.101574. Epub 2019 Oct 23.
Diagnosis of cancer through an emergency presentation is associated with worse clinical and patient experience outcomes. The proportion of patients with cancer who are diagnosed through emergency presentations has consequently been introduced as a routine cancer surveillance measure in England. Welcome reductions in this metric have been reported over more than a decade but whether reductions reflect true changes in how patients are diagnosed rather than the changing case-mix of incident cohorts in unknown.
We analysed 'Routes to Diagnosis' data on cancer patients (2006-2015) and used logistic regression modelling to determine the contribution of changes in four case-mix variables (sex, age, deprivation, cancer site) to time-trends in emergency presentations.
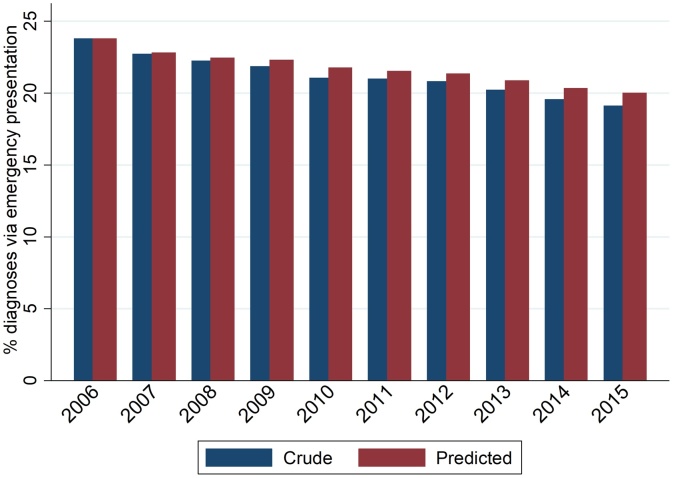
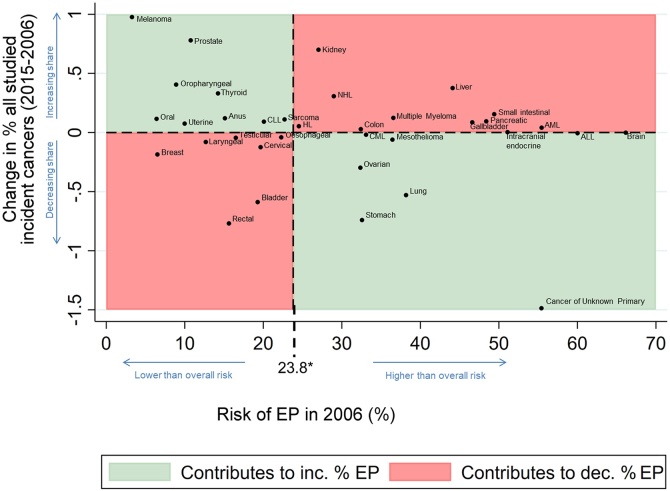
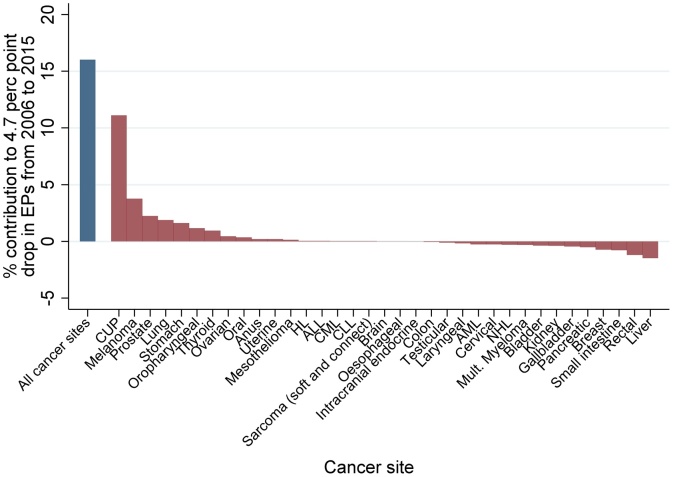
Between 2006 and 2015 there was an absolute 4.7 percentage point reduction in emergency presentations (23.8%-19.2%). Changing distributions of the four case-mix variables explained 19.0% of this reduction, leaving 81.0% unexplained. Changes in cancer site case-mix alone explained 16.0% of the total reduction.
Changes in case-mix (particularly that of cancer sites) account for about a fifth of the overall reduction in emergency presentations. This would support the use of adjustment/standardisation of reported statistics to support their interpretation and help appreciate the influence of case-mix, particularly regarding cancer sites with changing incidence. However, most of the reduction in emergency presentations remains unaccounted for, and likely reflects genuine changes during the study period in how patients were being diagnosed.
通过急诊就诊诊断癌症与更差的临床和患者体验结果相关。因此,在英国,通过急诊就诊诊断出的癌症患者比例已被纳入常规癌症监测措施。十多年来,该指标的降幅已得到报道,但降幅是否反映了患者诊断方式的真正变化,还是新发病例群体构成的变化尚不清楚。
我们分析了癌症患者的“诊断途径”数据(2006-2015 年),并使用逻辑回归模型来确定四个病例组合变量(性别、年龄、贫困程度、癌症部位)变化对急诊就诊时间趋势的贡献。
2006 年至 2015 年,急诊就诊绝对减少了 4.7 个百分点(23.8%-19.2%)。四个病例组合变量分布的变化解释了减少的 19.0%,其余 81.0%无法解释。仅癌症部位病例组合的变化就解释了总减少的 16.0%。
病例组合的变化(特别是癌症部位的变化)约占急诊就诊总体减少的五分之一。这将支持使用调整/标准化报告的统计数据来支持其解释,并有助于了解病例组合的影响,特别是关于发病率不断变化的癌症部位。然而,急诊就诊减少的大部分仍无法解释,这可能反映了研究期间患者诊断方式的真正变化。