National Disease Registration Service, NHS Digital, Leeds, UK.
National Disease Registration Service, NHS Digital, Leeds, UK; Cancer Research UK, London, UK.
Lancet Oncol. 2022 May;23(5):587-600. doi: 10.1016/S1470-2045(22)00127-9. Epub 2022 Apr 6.
Greater understanding of international cancer survival differences is needed. We aimed to identify predictors and consequences of cancer diagnosis through emergency presentation in different international jurisdictions in six high-income countries.
Using a federated analysis model, in this cross-sectional population-based study, we analysed cancer registration and linked hospital admissions data from 14 jurisdictions in six countries (Australia, Canada, Denmark, New Zealand, Norway, and the UK), including patients with primary diagnosis of invasive oesophageal, stomach, colon, rectal, liver, pancreatic, lung, or ovarian cancer during study periods from Jan 1, 2012, to Dec 31, 2017. Data were collected on cancer site, age group, sex, year of diagnosis, and stage at diagnosis. Emergency presentation was defined as diagnosis of cancer within 30 days after an emergency hospital admission. Using logistic regression, we examined variables associated with emergency presentation and associations between emergency presentation and short-term mortality. We meta-analysed estimates across jurisdictions and explored jurisdiction-level associations between cancer survival and the percentage of patients diagnosed as emergencies.
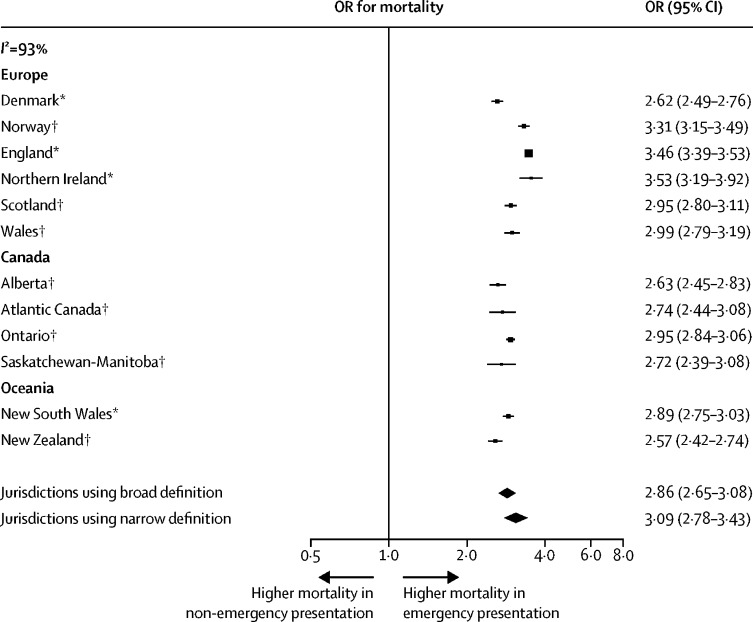
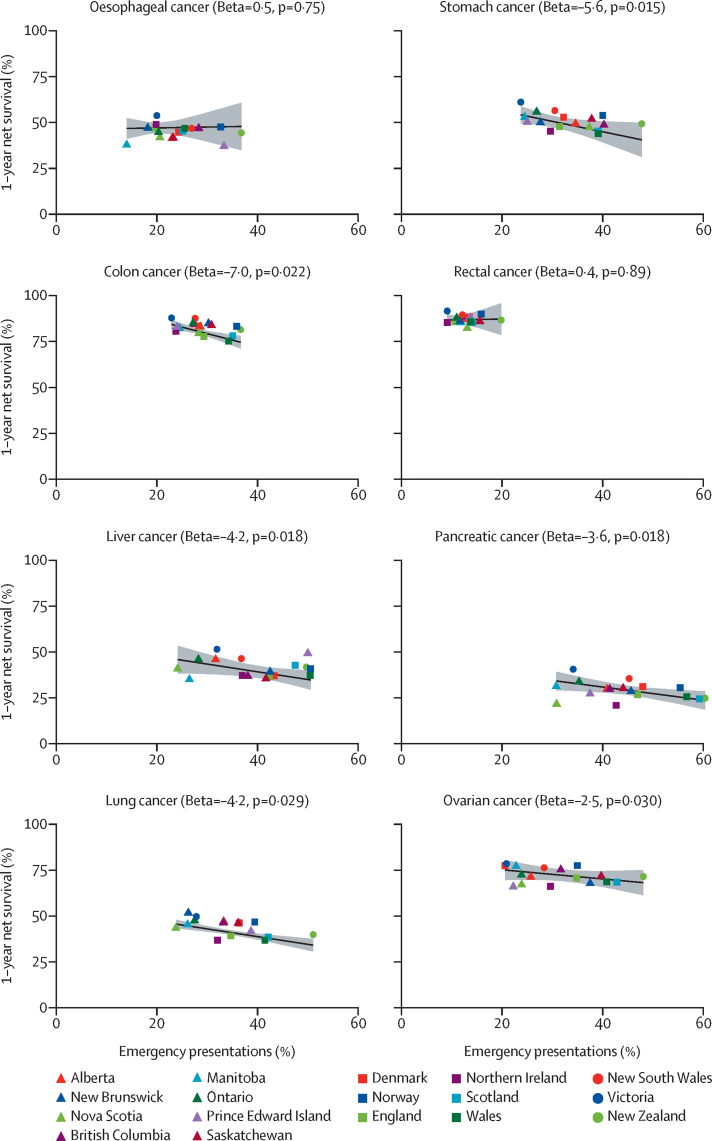
In 857 068 patients across 14 jurisdictions, considering all of the eight cancer sites together, the percentage of diagnoses through emergency presentation ranged from 24·0% (9165 of 38 212 patients) to 42·5% (12 238 of 28 794 patients). There was consistently large variation in the percentage of emergency presentations by cancer site across jurisdictions. Pancreatic cancer diagnoses had the highest percentage of emergency presentations on average overall (46·1% [30 972 of 67 173 patients]), with the jurisdictional range being 34·1% (1083 of 3172 patients) to 60·4% (1317 of 2182 patients). Rectal cancer had the lowest percentage of emergency presentations on average overall (12·1% [10 051 of 83 325 patients]), with a jurisdictional range of 9·1% (403 of 4438 patients) to 19·8% (643 of 3247 patients). Across the jurisdictions, older age (ie, 75-84 years and 85 years or older, compared with younger patients) and advanced stage at diagnosis compared with non-advanced stage were consistently associated with increased emergency presentation risk, with the percentage of emergency presentations being highest in the oldest age group (85 years or older) for 110 (98%) of 112 jurisdiction-cancer site strata, and in the most advanced (distant spread) stage category for 98 (97%) of 101 jurisdiction-cancer site strata with available information. Across the jurisdictions, and despite heterogeneity in association size (I=93%), emergency presenters consistently had substantially greater risk of 12-month mortality than non-emergency presenters (odds ratio >1·9 for 112 [100%] of 112 jurisdiction-cancer site strata, with the minimum lower bound of the related 95% CIs being 1·26). There were negative associations between jurisdiction-level percentage of emergency presentations and jurisdiction-level 1-year survival for colon, stomach, lung, liver, pancreatic, and ovarian cancer, with a 10% increase in percentage of emergency presentations in a jurisdiction being associated with a decrease in 1-year net survival of between 2·5% (95% CI 0·28-4·7) and 7·0% (1·2-13·0).
Internationally, notable proportions of patients with cancer are diagnosed through emergency presentation. Specific types of cancer, older age, and advanced stage at diagnosis are consistently associated with an increased risk of emergency presentation, which strongly predicts worse prognosis and probably contributes to international differences in cancer survival. Monitoring emergency presentations, and identifying and acting on contributing behavioural and health-care factors, is a global priority for cancer control.
Canadian Partnership Against Cancer; Cancer Council Victoria; Cancer Institute New South Wales; Cancer Research UK; Danish Cancer Society; National Cancer Registry Ireland; The Cancer Society of New Zealand; National Health Service England; Norwegian Cancer Society; Public Health Agency Northern Ireland, on behalf of the Northern Ireland Cancer Registry; the Scottish Government; Western Australia Department of Health; and Wales Cancer Network.
需要更深入地了解国际间癌症生存差异。本研究旨在确定在六个高收入国家的 14 个司法管辖区中,通过急诊就诊诊断癌症的预测因素和后果,这些司法管辖区包括澳大利亚、加拿大、丹麦、新西兰、挪威和英国。
本研究采用联邦分析模型,对来自六个国家的 14 个司法管辖区的癌症登记和相关医院入院数据进行了横断面人群研究,这些司法管辖区包括 2012 年 1 月 1 日至 2017 年 12 月 31 日期间确诊为侵袭性食管、胃、结肠、直肠、肝、胰腺、肺或卵巢癌的患者。数据收集了癌症部位、年龄组、性别、诊断年份和诊断时的分期。急诊诊断定义为在急诊入院后 30 天内诊断出癌症。使用逻辑回归分析了与急诊就诊相关的变量,并分析了急诊就诊与短期死亡率之间的关联。我们对各司法管辖区的估计值进行了荟萃分析,并探索了癌症生存率与作为急诊诊断的患者比例之间的司法管辖区关联。
在来自 14 个司法管辖区的 857068 名患者中,综合考虑所有 8 个癌症部位,通过急诊就诊诊断的比例范围为 24.0%(38212 名患者中的 9165 名)至 42.5%(28794 名患者中的 12238 名)。各司法管辖区的癌症部位急诊就诊比例存在显著差异。总体而言,胰腺癌诊断的急诊就诊比例最高(平均占 46.1%[67173 名患者中的 30972 名]),范围为 34.1%(3172 名患者中的 1083 名)至 60.4%(2182 名患者中的 1317 名)。直肠癌的急诊就诊比例最低(平均占 12.1%[83325 名患者中的 10051 名]),范围为 9.1%(4438 名患者中的 403 名)至 19.8%(4437 名患者中的 643 名)。在所有司法管辖区中,与年轻患者相比,年龄较大(即 75-84 岁和 85 岁及以上)和晚期诊断与非晚期诊断相比,与急诊就诊风险增加相关,在最年长的年龄组(85 岁及以上)中,急诊就诊比例最高(112 个司法管辖区-癌症部位分层中的 110 个,占 98%),在可获得信息的最晚期(远处转移)分期类别中,急诊就诊比例最高(101 个司法管辖区-癌症部位分层中的 98 个,占 97%)。在所有司法管辖区中,尽管关联大小存在异质性(I=93%),但急诊就诊者的 12 个月死亡率始终显著高于非急诊就诊者(112 个[100%]司法管辖区-癌症部位分层中的比值比>1.9,相关 95%CI 的最小下限为 1.26)。在结肠、胃、肺、肝、胰腺和卵巢癌中,各司法管辖区的急诊就诊比例与各司法管辖区的 1 年生存率呈负相关,在一个司法管辖区中,急诊就诊比例增加 10%,与 1 年净生存率下降 2.5%(95%CI 0.28-4.7)至 7.0%(1.2-13.0)相关。
在国际上,相当比例的癌症患者通过急诊就诊诊断。特定类型的癌症、年龄较大和晚期诊断与急诊就诊风险增加相关,这强烈预示着预后较差,可能是导致癌症生存国际差异的原因。监测急诊就诊情况,并识别和处理相关的行为和医疗保健因素,是全球癌症控制的重点。
加拿大癌症协会合作组织;维多利亚癌症委员会;新南威尔士癌症研究所;英国癌症研究协会;丹麦癌症协会;爱尔兰国家癌症登记处;新西兰癌症协会;英格兰国民保健署;挪威癌症协会;北爱尔兰公共卫生署(代表北爱尔兰癌症登记处);苏格兰政府;西澳大利亚州卫生部;威尔士癌症网络。