Department of Neurosurgery Brigham and Women's Hospital Harvard Medical School Boston MA.
J Am Heart Assoc. 2019 Nov 5;8(21):e013412. doi: 10.1161/JAHA.119.013412. Epub 2019 Oct 30.
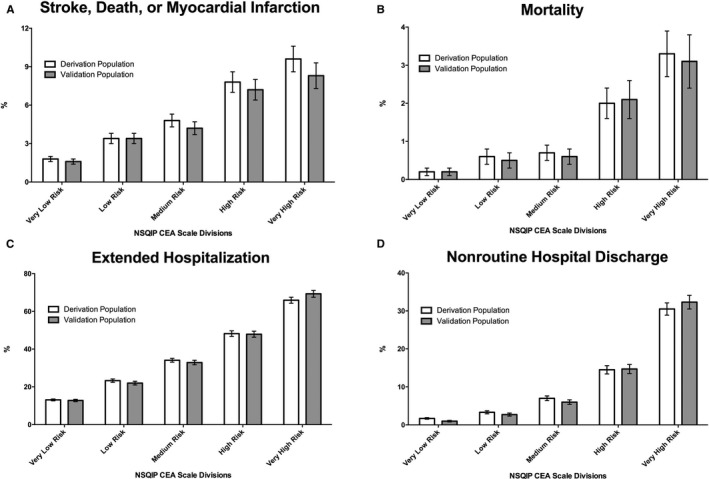
Background The goal of this study was to create a comprehensive, integer-weighted predictive scale of adverse events after carotid endarterectomy (CEA), which may augment risk stratification and patient counseling. Methods and Results The targeted carotid files from the prospective NSQIP (National Surgical Quality Improvement Program) registry (2011-2013) comprised the derivation population. Multivariable logistic regression evaluated predictors of a 30-day adverse event (stroke, myocardial infarction, or death), the effect estimates of which were used to build a weighted predictive scale that was validated using the 2014 to 2015 NSQIP registry release. A total of 10 766 and 8002 patients were included in the derivation and the validation populations, in whom 4.0% and 3.7% developed an adverse event, respectively. The NSQIP registry CEA scale included 14 variables; the highest points were allocated for insulin-dependent diabetes mellitus, high-risk cardiac physiological characteristics, admission source other than home, an emergent operation, American Society of Anesthesiologists' classification IV to V, modified Rankin Scale score ≥2, and presentation with a stroke. NSQIP registry CEA score was predictive of an adverse event (concordance=0.67), stroke or death (concordance=0.69), mortality (concordance=0.76), an extended hospitalization (concordance=0.73), and a nonroutine discharge (concordance=0.83) in the validation population, as well as among symptomatic and asymptomatic subgroups (<0.001). In the validation population, patients with an NSQIP registry CEA scale score >8 and 17 had 30-day stroke or death rates >3% and 6%, the recommended thresholds for asymptomatic and symptomatic patients, respectively. Conclusions The NSQIP registry CEA scale predicts adverse outcomes after CEA and can risk stratify patients with both symptomatic and asymptomatic carotid stenosis using different thresholds for each population.
背景 本研究旨在创建一个全面的、整数加权的颈动脉内膜切除术(CEA)后不良事件预测量表,以增强风险分层和患者咨询。
方法和结果 从前瞻性 NSQIP(国家手术质量改进计划)登记处(2011-2013 年)的目标颈动脉文件中获得了推导人群。多变量逻辑回归评估了 30 天不良事件(中风、心肌梗死或死亡)的预测因素,这些预测因素的效应估计值用于构建加权预测量表,然后使用 2014 年至 2015 年 NSQIP 登记处发布的数据进行验证。推导人群和验证人群分别纳入了 10766 例和 8002 例患者,其中分别有 4.0%和 3.7%的患者发生了不良事件。NSQIP 登记处的 CEA 量表包含 14 个变量;最高分数分配给依赖胰岛素的糖尿病、高危心脏生理特征、非家庭入院来源、紧急手术、美国麻醉师协会分类 IV 至 V 级、改良 Rankin 量表评分≥2 分以及中风发作。NSQIP 登记处的 CEA 评分可预测不良事件(一致性=0.67)、中风或死亡(一致性=0.69)、死亡率(一致性=0.76)、延长住院时间(一致性=0.73)和非常规出院(一致性=0.83),在验证人群中,以及在有症状和无症状亚组中(<0.001)。在验证人群中,NSQIP 登记处的 CEA 评分>8 和 17 的患者在 30 天内发生中风或死亡的风险率分别>3%和 6%,这是无症状和有症状患者的推荐阈值。
结论 NSQIP 登记处的 CEA 量表预测 CEA 后的不良结果,并可使用每个人群的不同阈值对有症状和无症状颈动脉狭窄的患者进行风险分层。