Bonelli Patrizia, Borrelli Antonella, Tuccillo Franca Maria, Silvestro Lucrezia, Palaia Raffaele, Buonaguro Franco Maria
Molecular Biology and Viral Oncology, Istituto Nazionale Tumori - IRCCS - Fondazione G Pascale, Napoli 80131, Italy.
Abdominal Medical Oncology, Istituto Nazionale Tumori - IRCCS - Fondazione G Pascale, Napoli 80131, Italy.
World J Gastrointest Oncol. 2019 Oct 15;11(10):804-829. doi: 10.4251/wjgo.v11.i10.804.
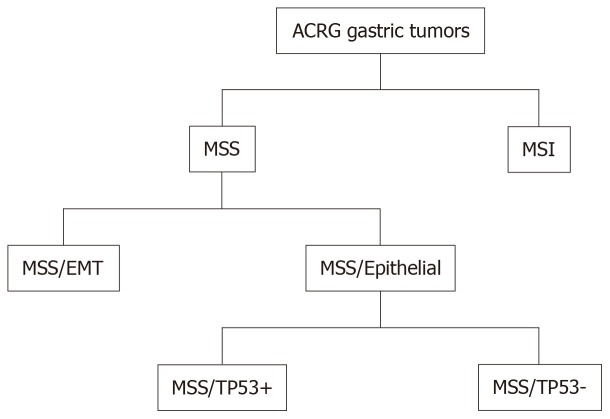
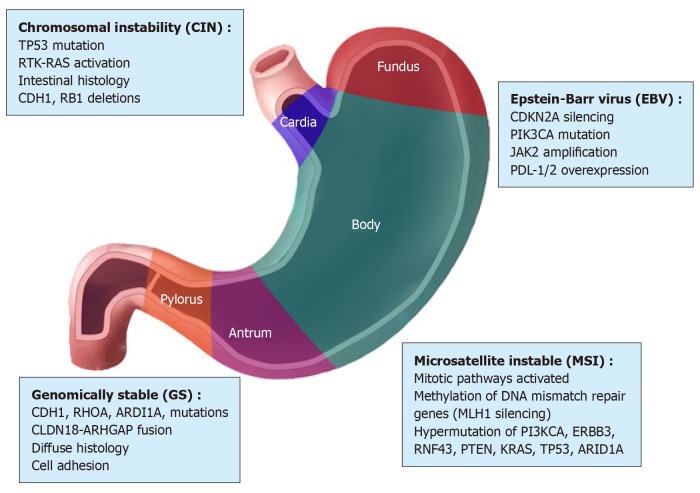
Gastric cancer (GC) is a complex disease linked to a series of environmental factors and unhealthy lifestyle habits, and especially to genetic alterations. GC represents the second leading cause of cancer-related deaths worldwide. Its onset is subtle, and the majority of patients are diagnosed once the cancer is already advanced. In recent years, there have been innovations in the management of advanced GC including the introduction of new classifications based on its molecular characteristics. Thanks to new technologies such as next-generation sequencing and microarray, the Cancer Genome Atlas and Asian Cancer Research Group classifications have also paved the way for precision medicine in GC, making it possible to integrate diagnostic and therapeutic methods. Among the objectives of the subdivision of GC into subtypes is to select patients in whom molecular targeted drugs can achieve the best results; many lines of research have been initiated to this end. After phase III clinical trials, trastuzumab, anti-Erb-B2 receptor tyrosine kinase 2 (commonly known as ERBB2) and ramucirumab, anti-vascular endothelial growth factor receptor 2 (commonly known as VEGFR2) monoclonal antibodies, were approved and introduced into first- and second-line therapies for patients with advanced/metastatic GC. However, the heterogeneity of this neoplasia makes the practical application of such approaches difficult. Unfortunately, scientific progress has not been matched by progress in clinical practice in terms of significant improvements in prognosis. Survival continues to be low in contrast to the reduction in deaths from many common cancers such as colorectal, lung, breast, and prostate cancers. Although several target molecules have been identified on which targeted drugs can act and novel products have been introduced into experimental therapeutic protocols, the overall approach to treating advanced stage GC has not substantially changed. Currently, surgical resection with adjuvant or neoadjuvant radiotherapy and chemotherapy are the most effective treatments for this disease. Future research should not underestimate the heterogeneity of GC when developing diagnostic and therapeutic strategies aimed toward improving patient survival.
胃癌(GC)是一种与一系列环境因素和不健康生活习惯相关的复杂疾病,尤其与基因改变有关。胃癌是全球癌症相关死亡的第二大主要原因。其发病较为隐匿,大多数患者在癌症已进展到晚期时才被诊断出来。近年来,晚期胃癌的治疗有了创新,包括基于分子特征引入新的分类方法。得益于下一代测序和微阵列等新技术,癌症基因组图谱和亚洲癌症研究小组的分类也为胃癌的精准医学铺平了道路,使整合诊断和治疗方法成为可能。将胃癌细分为亚型的目标之一是选择分子靶向药物能取得最佳效果的患者;为此已经启动了许多研究项目。经过III期临床试验后,曲妥珠单抗(抗Erb-B2受体酪氨酸激酶2,通常称为ERBB2)和雷莫西尤单抗(抗血管内皮生长因子受体2,通常称为VEGFR2)单克隆抗体被批准并引入晚期/转移性胃癌患者的一线和二线治疗。然而,这种肿瘤的异质性使得这些方法的实际应用变得困难。不幸的是,在临床实践中,科学进展并未在预后的显著改善方面与之匹配。与结直肠癌、肺癌、乳腺癌和前列腺癌等许多常见癌症的死亡人数减少形成对比的是,胃癌患者的生存率仍然很低。尽管已经确定了几种靶向药物可以作用的靶分子,并且新的产品已被引入实验性治疗方案中,但治疗晚期胃癌的总体方法并未发生实质性改变。目前对于这种疾病,手术切除联合辅助或新辅助放疗及化疗是最有效的治疗方法。在制定旨在提高患者生存率的诊断和治疗策略时,未来的研究不应低估胃癌的异质性。