Analysis Group, Inc, Montréal, Québec, Canada.
Janssen Scientific Affairs, LLC, Horsham, PA.
Clin Lymphoma Myeloma Leuk. 2019 Dec;19(12):763-775.e2. doi: 10.1016/j.clml.2019.08.004. Epub 2019 Aug 26.
Studies assessing ibrutinib's economic burden versus chemoimmunotherapy (CIT) focused on pharmacy costs but not medical costs. This study compared time to next treatment (TTNT), health care resource utilization (HRU), and total direct costs among patients with chronic lymphocytic leukemia (CLL) initiating front-line ibrutinib single agent (Ibr) or CIT.
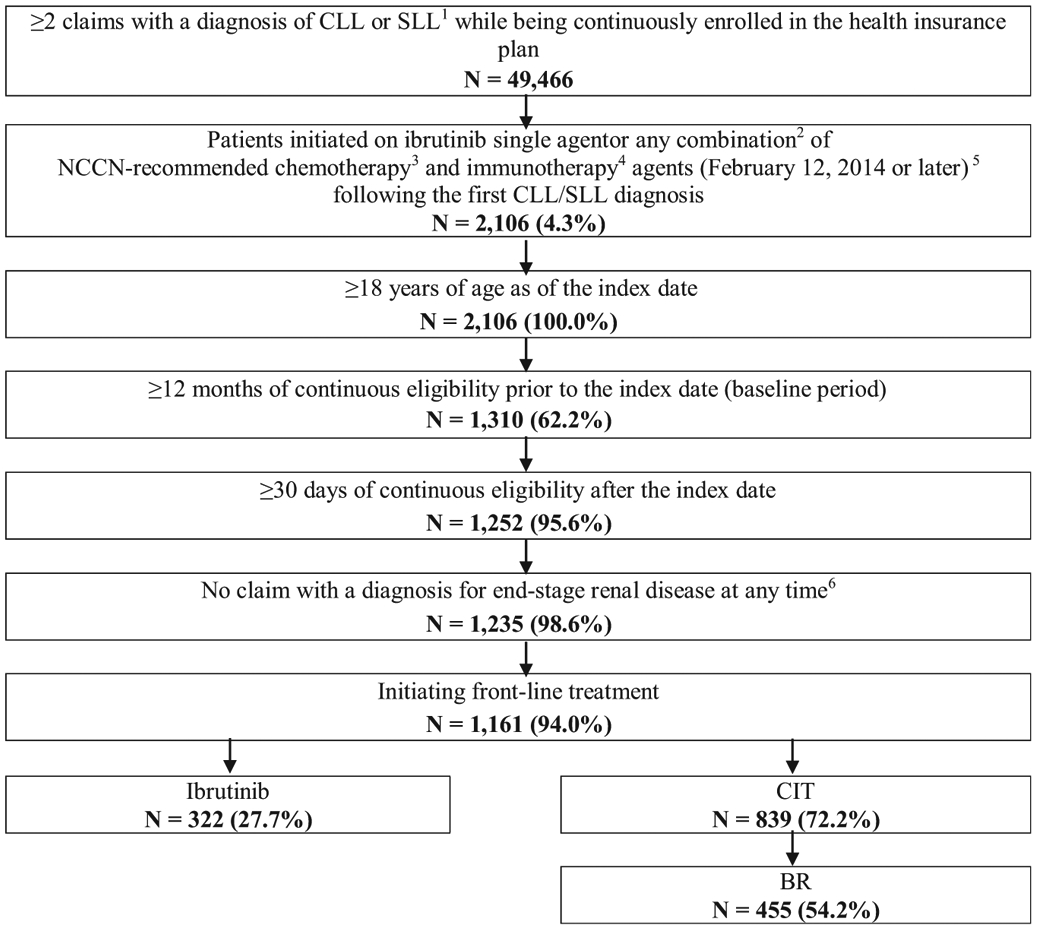
Optum Clinformatics Extended DataMart De-Identified Databases were used to identify adults with ≥ 2 claims with a CLL diagnosis initiating front-line Ibr or CIT from February 12, 2014 to June 30, 2017. Inverse probability of treatment weighting was used to control for potential differences in baseline characteristics between the Ibr and CIT cohorts. Two periods were considered: entire front-line therapy (until initiation of second-line therapy) and first 6 months of front-line therapy. Comparisons with a subgroup of CIT patients initiating bendamustine/rituximab (BR) were also conducted.
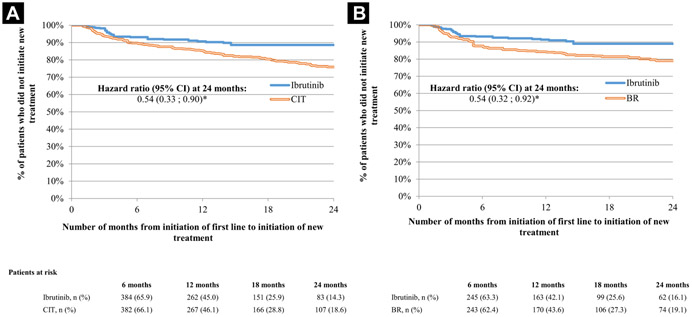
TTNT was significantly longer for Ibr (N = 322) relative to CIT (N = 839; hazard ratio, 0.54; P = .0163; Kaplan-Meier rates [24 months]: Ibr = 88.6%, CIT = 75.9%) and the subset of CIT patients treated with BR (N = 455; hazard ratio, 0.54; P = .0208; Kaplan-Meier rates [24 months]: Ibr = 89.0%, BR = 79.0%). During the entire front-line therapy, Ibr patients had significantly fewer monthly days with outpatient visits (rate ratio = 0.75; P = .0200). Ibrutinib's higher pharmacy costs (mean monthly cost difference [MMCD] = $6,849; P < .0001) were offset by lower medical costs (MMCD = -$10,615; P < .0001), yielding net savings (MMCD = -$3,766; P < .0001) versus CIT. Ibr was associated with net savings (MMCD = -$5,569; P < .0001) versus BR. Cost savings and reductions in HRU were more pronounced during the first 6 months of front-line therapy.
During front-line CLL treatment, Ibr was associated with longer TTNT, fewer monthly days with outpatient visits, and net monthly total cost reduction versus CIT and BR.
评估伊布替尼(ibrutinib)的经济负担与化疗免疫治疗(CIT)的研究主要关注药房成本,而不关注医疗成本。本研究比较了初治慢性淋巴细胞白血病(CLL)患者使用伊布替尼单药(Ibr)或 CIT 时的无进展生存时间(TTNT)、卫生保健资源利用(HRU)和总直接成本。
利用 Optum Clinformatics 扩展数据集市去标识数据库,筛选 2014 年 2 月 12 日至 2017 年 6 月 30 日期间至少有 2 次 CLL 诊断记录且初治的成年患者。采用逆概率治疗加权法控制 Ibr 和 CIT 队列间基线特征的潜在差异。考虑了两个时间段:整个一线治疗(直至二线治疗开始)和一线治疗的前 6 个月。还与接受苯达莫司汀/利妥昔单抗(BR)治疗的 CIT 患者亚组进行了比较。
与 CIT(N=839)相比,Ibr(N=322)的 TTNT 显著延长(风险比,0.54;P=0.0163;24 个月 Kaplan-Meier 率:Ibr=88.6%,CIT=75.9%),且与接受 BR 治疗的 CIT 患者亚组(N=455)相比(风险比,0.54;P=0.0208;24 个月 Kaplan-Meier 率:Ibr=89.0%,BR=79.0%)。在整个一线治疗期间,Ibr 患者的门诊就诊月天数显著减少(月就诊率比,0.75;P=0.0200)。Ibrutinib 的较高药房成本(每月成本差异均值 [MMCD],6849 美元;P<0.0001)被较低的医疗成本(MMCD,-10615 美元;P<0.0001)所抵消,与 CIT 相比,产生了净节省(MMCD,-3766 美元;P<0.0001)。与 BR 相比,Ibr 也产生了净节省(MMCD,-5569 美元;P<0.0001)。在一线治疗的前 6 个月,成本节省和 HRU 减少更为显著。
在初治 CLL 治疗中,与 CIT 和 BR 相比,Ibr 与 TTNT 延长、门诊就诊月天数减少和每月总直接成本降低有关。