Wagstaff Jadon S, Durrant Robert J, Newman Michael G, Eason Rachael, Ward Robert M, Sherwin Catherine M T, Enioutina Elena Y
Division of Clinical Pharmacology, Department of Pediatrics, University of Utah School of Medicine, Salt Lake City, UT, United States.
Division of Medical Laboratory Science, Department of Pathology, School of Medicine, University of Utah, Salt Lake City, UT, United States.
Front Pharmacol. 2019 Oct 15;10:1191. doi: 10.3389/fphar.2019.01191. eCollection 2019.
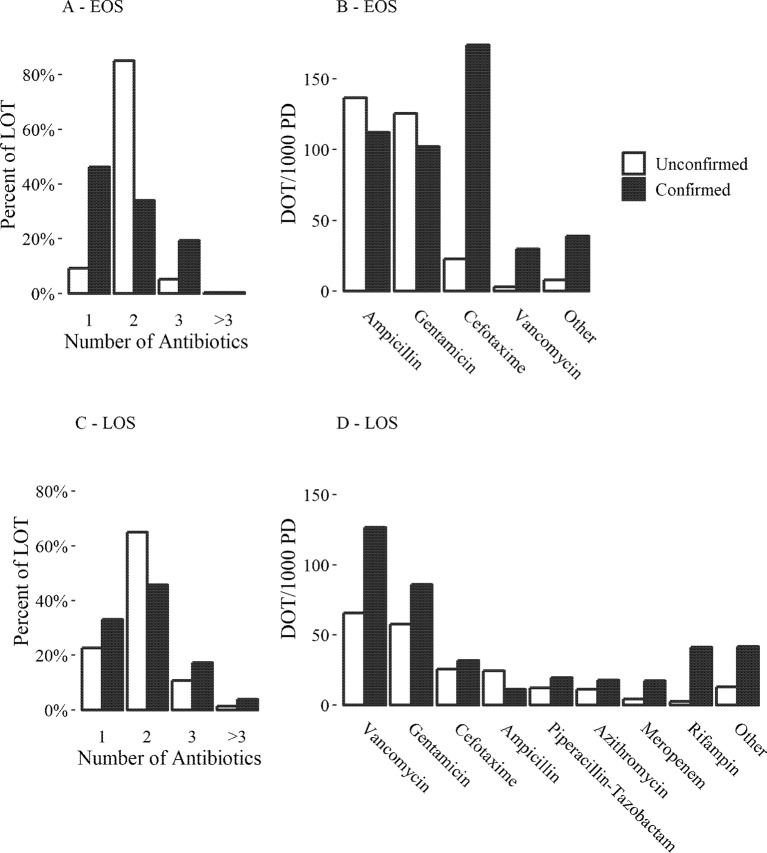
Neonatal sepsis causes significant mortality and morbidity worldwide. Diagnosis is usually confirmed blood culture results. Blood culture sepsis confirmation can take days and suffer from contamination and false negatives. Empiric therapy with antibiotics is common. This study aims to retrospectively describe and compare treatments of blood culture-confirmed and unconfirmed, but suspected, sepsis within the University of Utah Hospital system. Electronic health records were obtained from 1,248 neonates from January 1, 2006, to December 31, 2017. Sepsis was categorized into early-onset (≤3 days of birth, EOS) and late-onset (>3 and ≤28 days of birth, LOS) and categorized as culture-confirmed sepsis if a pathogen was cultured from the blood and unconfirmed if all blood cultures were negative with no potentially contaminated blood cultures. Of 1,010 neonates in the EOS cohort, 23 (2.3%) were culture-confirmed, most with (42%). Treatment for unconfirmed EOS lasted an average of 6.1 days with primarily gentamicin and ampicillin while confirmed patients were treated for an average of 12.3 days with increased administration of cefotaxime. Of 311 neonates in the LOS cohort, 62 (20%) were culture-confirmed, most culturing coagulase negative staphylococci (46%). Treatment courses for unconfirmed LOS lasted an average of 7.8 days while confirmed patients were treated for an average of 11.4 days, these patients were primarily treated with vancomycin and gentamicin. The use of cefotaxime for unconfirmed EOS and LOS increased throughout the study period. Cefotaxime administration was associated with an increase in neonatal mortality, even when potential confounding factors were added to the logistic regression model (adjusted odds ratio 2.8, 95%CI [1.21, 6.88], p = 0.02). These results may not be generalized to all hospitals and the use of cefotaxime may be a surrogate for other factors. Given the low rate of blood culture positive diagnosis and the high exposure rate of empiric antibiotics, this patient population might benefit from improved diagnostics with reevaluation of antibiotic use guidelines.
新生儿败血症在全球范围内导致了显著的死亡率和发病率。诊断通常通过血培养结果来确认。血培养确诊败血症可能需要数天时间,且存在污染和假阴性问题。使用抗生素进行经验性治疗很常见。本研究旨在回顾性描述和比较犹他大学医院系统内血培养确诊和未确诊但疑似败血症的治疗情况。从2006年1月1日至2017年12月31日的1248名新生儿中获取了电子健康记录。败血症分为早发型(出生≤3天,EOS)和晚发型(出生>3天且≤28天,LOS),如果从血液中培养出病原体则归类为血培养确诊败血症,如果所有血培养均为阴性且无潜在污染的血培养则归类为未确诊。在EOS队列的1010名新生儿中,23名(2.3%)血培养确诊,大多数为革兰氏阴性菌(42%)。未确诊EOS的治疗平均持续6.1天,主要使用庆大霉素和氨苄西林,而确诊患者平均治疗12.3天,头孢噻肟的使用增加。在LOS队列的311名新生儿中,62名(20%)血培养确诊,大多数培养出凝固酶阴性葡萄球菌(46%)。未确诊LOS的治疗疗程平均持续7.8天,而确诊患者平均治疗11.4天,这些患者主要接受万古霉素和庆大霉素治疗。在整个研究期间,未确诊EOS和LOS使用头孢噻肟的情况有所增加。头孢噻肟的使用与新生儿死亡率增加相关,即使在逻辑回归模型中加入潜在混杂因素后也是如此(调整后的优势比为2.8,95%CI[1.21, 6.88],p = 0.02)。这些结果可能无法推广到所有医院,头孢噻肟的使用可能是其他因素的替代指标。鉴于血培养阳性诊断率低和经验性抗生素暴露率高,该患者群体可能会从改进诊断和重新评估抗生素使用指南中受益。