University Hospital Tuebingen, Tuebingen, Germany.
Helios Klinikum Pforzheim, Pforzheim, Germany.
BMC Surg. 2019 Nov 5;19(1):160. doi: 10.1186/s12893-019-0625-2.
Electrosurgical vessel sealers are gradually replacing conventional techniques such as ligation and clipping. Algorithms that control electrosurgical units (ESU), known as modes, are important for applications in different surgical disciplines. This chronic porcine animal study aimed to evaluate the safety and effectiveness of the novel thermoSEAL electrosurgical vessel sealing mode (TSM). The BiClamp® mode (BCM) of the renowned VIO® 300 D ESU served as control. BCM has been widely available since 2002 and has since been successfully used in many surgical disciplines. The TSM, for the novel VIO® 3 ESU, was developed to reduce sealing time and/or thermal lateral spread adjacent to the seal while maintaining clinical success rates. The primary aim of this study was to investigate the long-term and intraoperative seal quality of TSM.
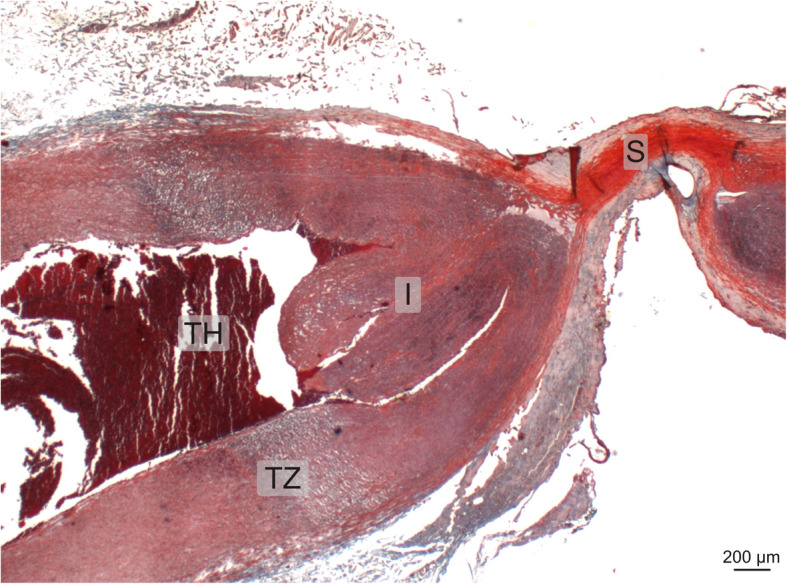
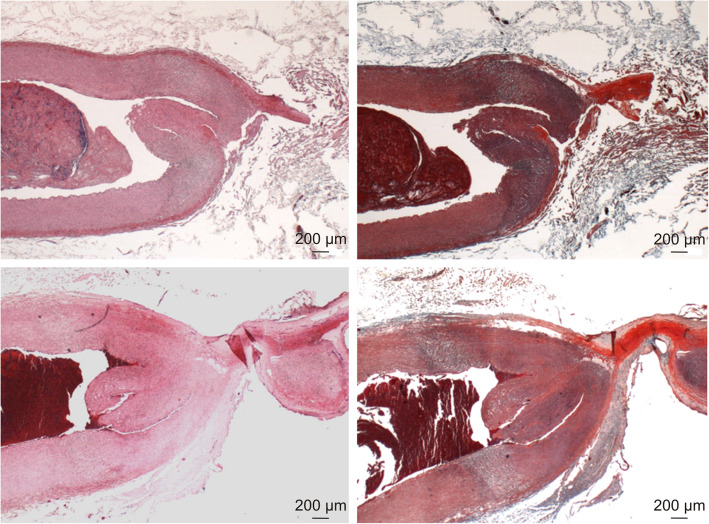
The BiCision® device was used for vessel sealing with TSM and BCM in ten German Landrace pigs which underwent splenectomy and unilateral nephrectomy during the first intervention of the study. The seals were cut with the BiCision® knife. Ninety-nine arteries, veins and vascular bundles were chronically sealed for 5 or 21 days. Thereafter, during the second and terminal intervention of the study, 97 additional arteries and veins were sealed. The carotid arteries were used for histological evaluation of thermal spread.
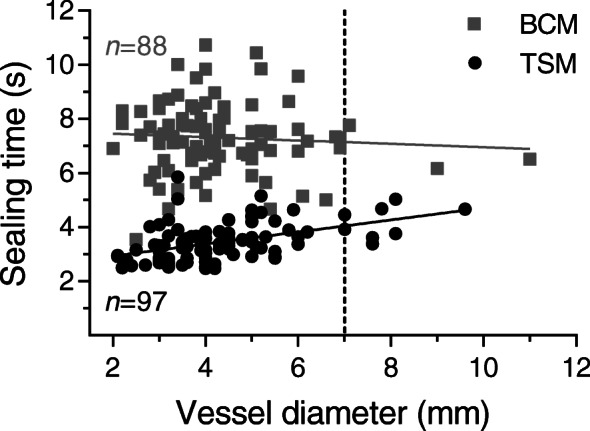
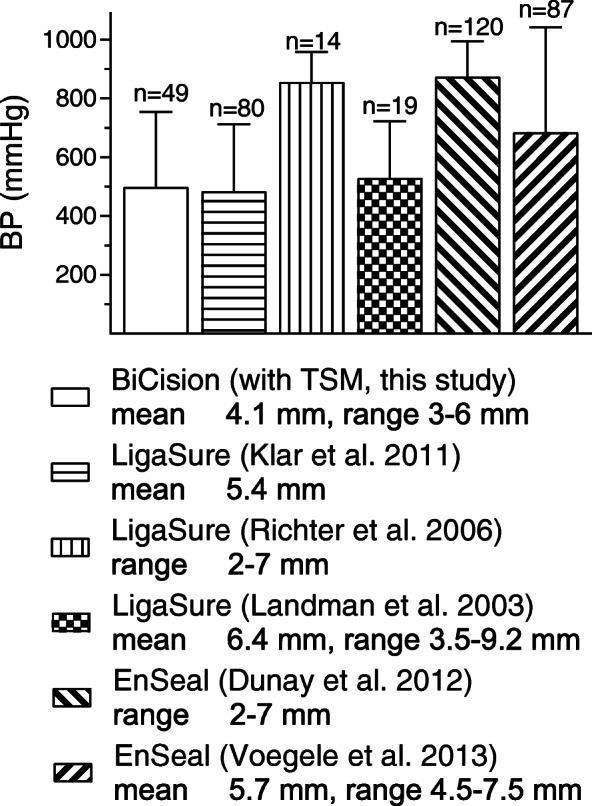
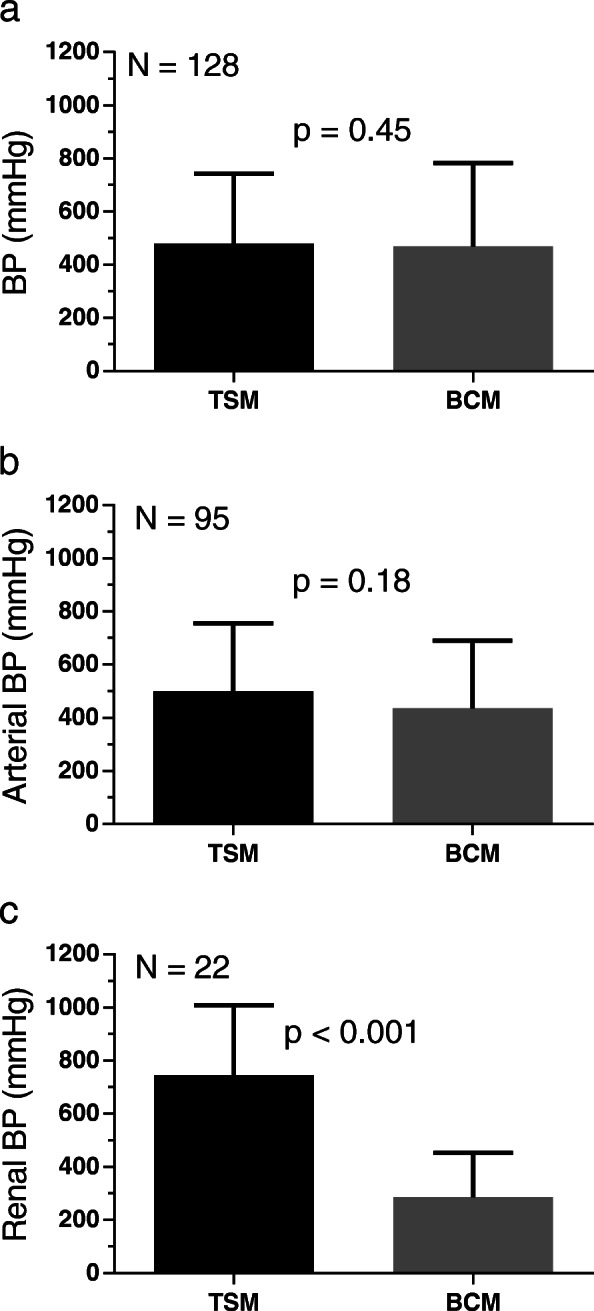
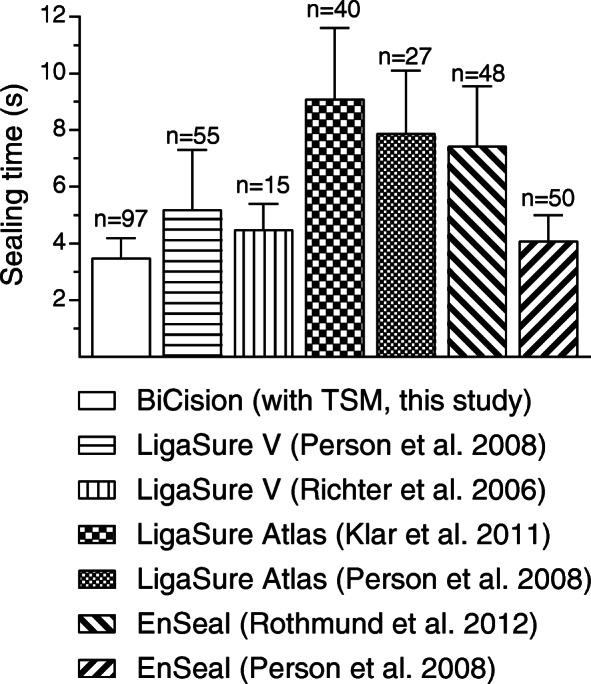
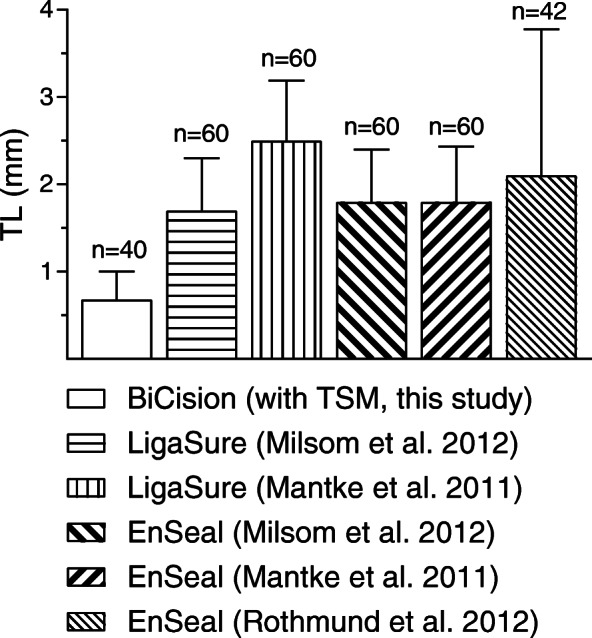
After each survival period, no long-term complications occurred with either mode. The intraoperative seal failure rates, i.e. vessel leaking or residual blood flow after the first sealing activation, were 2% with TSM versus 6% with BCM (p = 0.28). The sealing time was significantly shorter with TSM (3.5 ± 0.69 s vs. 7.3 ± 1.3 s, p < 0.0001). The thermal spread and burst pressure of arteries sealed with both modes were similar (p = 0.18 and p = 0.61) and corresponded to the histological evaluation. The measured tissue sticking parameter was rare with both modes (p = 0.33). Tissue charring did not occur. Regarding the cut quality, 97% of the seals were severed in the first and 3% in the second attempt (both with TSM and BCM).
The novel TSM seals blood vessels twice as fast as the BCM while maintaining excellent tissue effect and clinical success rates.
Not applicable.
电外科血管密封器逐渐取代传统的结扎和夹闭技术。控制电外科单元(ESU)的算法,即所谓的模式,对于不同外科学科的应用非常重要。这项针对慢性猪的动物研究旨在评估新型热 SEAL 电外科血管密封模式(TSM)的安全性和有效性。著名的 VIO® 300 D ESU 的 BiClamp®模式(BCM)作为对照。BCM 自 2002 年以来广泛应用,并已成功应用于许多外科学科。为了减少密封时间和/或密封相邻组织的热侧向扩散,同时保持临床成功率,为新型 VIO® 3 ESU 开发了 TSM。本研究的主要目的是研究 TSM 的长期和术中密封质量。
在这项研究的第一次干预中,使用 BiCision®设备通过 TSM 和 BCM 在 10 只德国长白猪中进行血管密封,这些猪接受了脾切除术和单侧肾切除术。密封后用 BiCision®刀切割。99 条动脉、静脉和血管束被慢性密封 5 或 21 天。此后,在研究的第二次和终末干预中,又密封了 97 条额外的动脉和静脉。用颈动脉评估热扩散的组织学。
在每个存活期后,两种模式均未发生长期并发症。术中密封失败率,即第一次密封激活后血管泄漏或残留血流,TSM 为 2%,BCM 为 6%(p=0.28)。TSM 的密封时间明显更短(3.5±0.69 秒 vs. 7.3±1.3 秒,p<0.0001)。两种模式密封的动脉热扩散和爆裂压力相似(p=0.18 和 p=0.61),与组织学评估结果一致。两种模式的组织粘连参数都很少见(p=0.33)。没有发生组织碳化。至于切割质量,97%的密封在第一次尝试中被切断,3%的密封在第二次尝试中被切断(TSM 和 BCM 都是)。
新型 TSM 密封血管的速度是 BCM 的两倍,同时保持了出色的组织效果和临床成功率。
不适用。