Division of Gastroenterology and Hepatology, Department of Internal Medicine III, Medical University of Vienna, Vienna, Austria.
Vienna Hepatic Hemodynamic Laboratory, Medical University of Vienna, Vienna, Austria.
PLoS One. 2019 Nov 6;14(11):e0224506. doi: 10.1371/journal.pone.0224506. eCollection 2019.
Studies in animal models have suggested that hepatic steatosis impacts on portal pressure, potentially by inducing liver sinusoidal endothelial dysfunction and thereby increasing intrahepatic resistance. Thus, we aimed to evaluate the impact of hepatic steatosis on hepatic venous pressure gradient (HVPG) in patients with chronic liver disease.
261 patients undergoing simultaneous HVPG measurements and controlled attenuation parameter (CAP)-based steatosis assessment were included in this retrospective study.
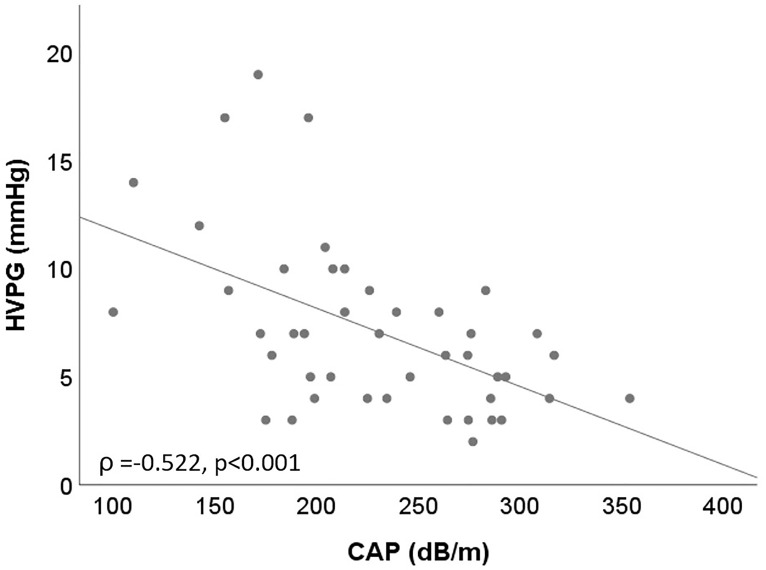
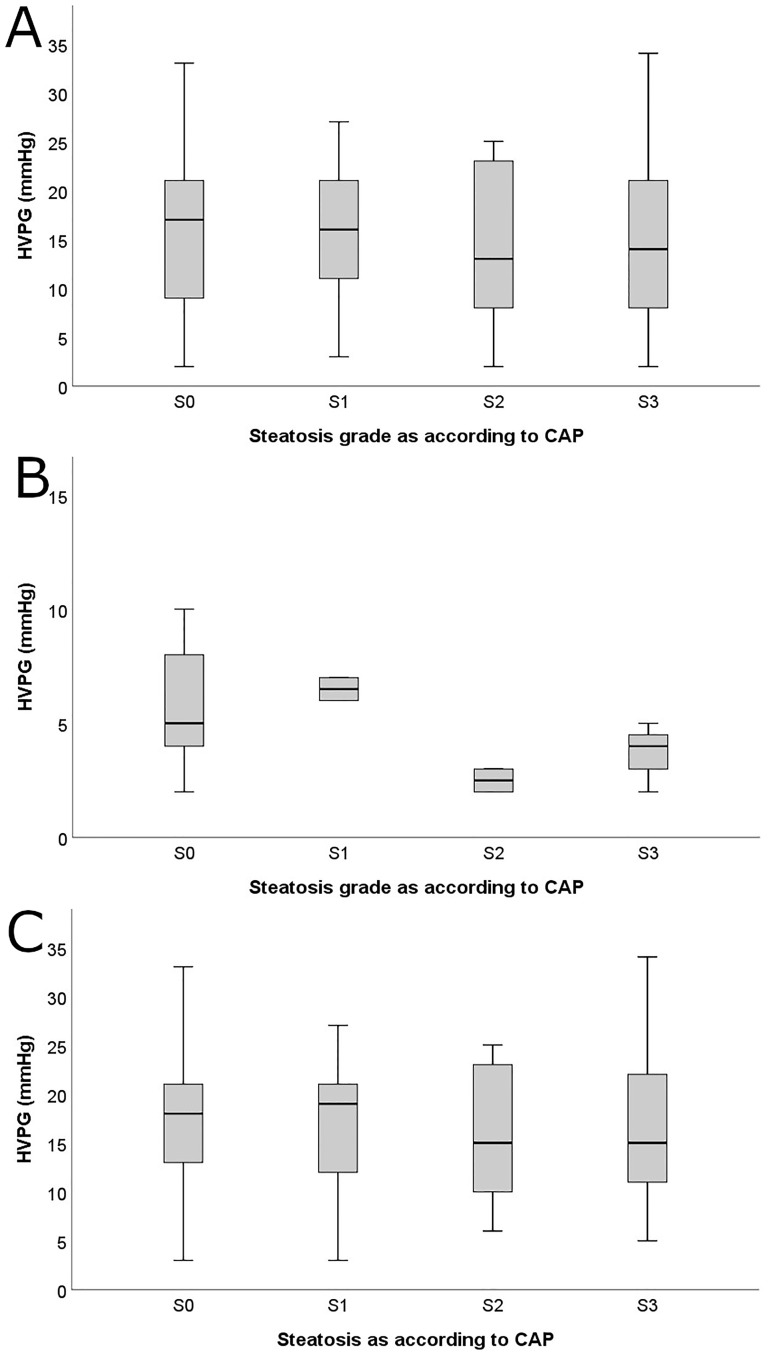
The majority of patients had cirrhosis (n = 205; 78.5%) and n = 191 (73.2%) had clinically significant portal hypertension (CSPH; HVPG≥10mmHg). Hepatic steatosis (S1/2/3; CAP ≥248dB/m) was present in n = 102 (39.1%). Overall, HVPG was comparable between patients with vs. without hepatic steatosis (15.5±7.5 vs. 14.8±7.7mmHg; p = 0.465). Neither in patients with HVPG (<6mmHg; p = 0.371) nor in patients with mild portal hypertension (HVPG 6-9mmHg; p = 0.716) or CSPH (HVPG≥10mmHg; p = 0.311) any correlation between CAP and HVPG was found. Interestingly, in patients with liver fibrosis F2/3, there was a negative correlation between CAP and HVPG (Pearson's ρ:-0.522; p≤0.001). In multivariate analysis, higher CAP was an independent 'protective' factor for the presence of CSPH (odds ratio [OR] per 10dB/m: 0.92, 95% confidence interval [CI]:0.85-1.00; p = 0.045), while liver stiffness was associated with the presence of CSPH (OR per kPa: 1.26, 95%CI: 1.17-1.36; p≤0.001). In 78 patients, in whom liver biopsy was performed, HVPG was neither correlated with percentage of histological steatosis (p = 0.714) nor with histological steatosis grade (p = 0.957).
Hepatic steatosis, as assessed by CAP and liver histology, did not impact on HVPG in our cohort comprising a high proportion of patients with advanced chronic liver disease. However, high CAP values (i.e. pronounced hepatic steatosis) might lead to overestimation of liver fibrosis by 'artificially' increasing transient elastography-based liver stiffness measurements.
动物模型研究表明,肝脂肪变性会影响门静脉压力,可能通过诱导肝窦内皮功能障碍从而增加肝内阻力。因此,我们旨在评估肝脂肪变性对慢性肝病患者肝静脉压力梯度(HVPG)的影响。
本回顾性研究纳入了 261 例同时接受 HVPG 测量和受控衰减参数(CAP)为基础的脂肪变性评估的患者。
大多数患者患有肝硬化(n=205;78.5%),191 例(73.2%)存在临床显著门静脉高压(CSPH;HVPG≥10mmHg)。102 例(39.1%)存在肝脂肪变性(S1/2/3;CAP≥248dB/m)。总体而言,有肝脂肪变性患者的 HVPG 与无肝脂肪变性患者的 HVPG 无差异(15.5±7.5 与 14.8±7.7mmHg;p=0.465)。在 HVPG<6mmHg(p=0.371)、6-9mmHg(p=0.716)或≥10mmHg(p=0.311)的患者中,CAP 与 HVPG 之间均无相关性。有趣的是,在纤维化程度为 F2/3 的患者中,CAP 与 HVPG 呈负相关(Pearson ρ:-0.522;p≤0.001)。多变量分析显示,CAP 每增加 10dB/m,CSPH 的存在几率呈独立的“保护”趋势(优势比[OR]每 10dB/m:0.92,95%置信区间[CI]:0.85-1.00;p=0.045),而肝脏硬度与 CSPH 的存在相关(每千帕 OR:1.26,95%CI:1.17-1.36;p≤0.001)。在 78 例行肝活检的患者中,HVPG 与组织学脂肪变性的百分比(p=0.714)或组织学脂肪变性分级(p=0.957)均无相关性。
在本研究纳入的大多数为晚期慢性肝病患者的队列中,CAP 和肝组织学评估的肝脂肪变性并不影响 HVPG。然而,高 CAP 值(即明显的肝脂肪变性)可能会通过“人为”增加基于瞬时弹性成像的肝脏硬度测量值,导致对肝纤维化的高估。