Shah Darshan S, Bates Taylor, Fowler Justin, Osborn Patrick, Jorgensen Anton Y
Orthopaedic Surgery, San Antonio Military Medical Center, San Antonio, USA.
Cureus. 2019 Sep 11;11(9):e5621. doi: 10.7759/cureus.5621.
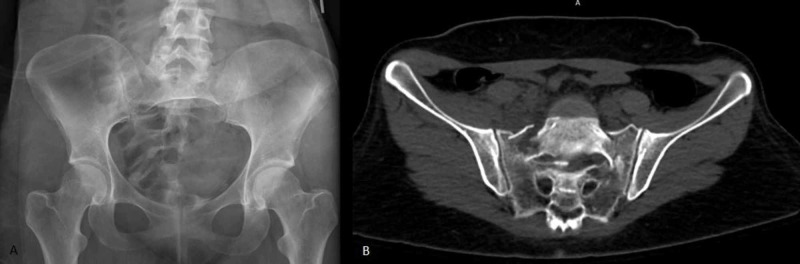
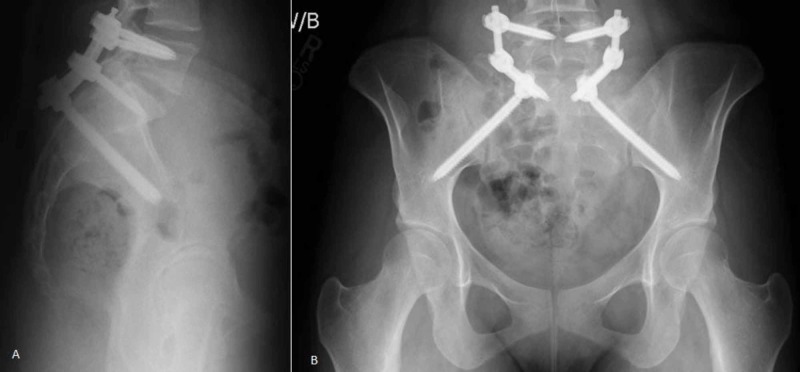
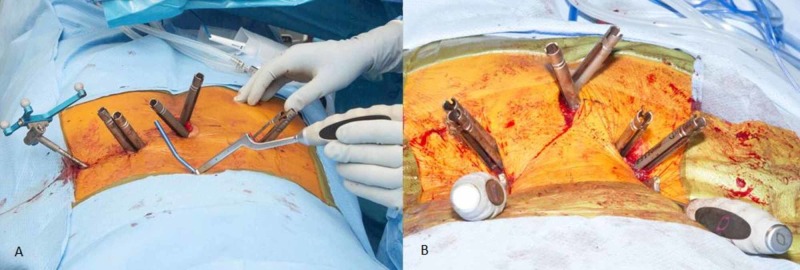
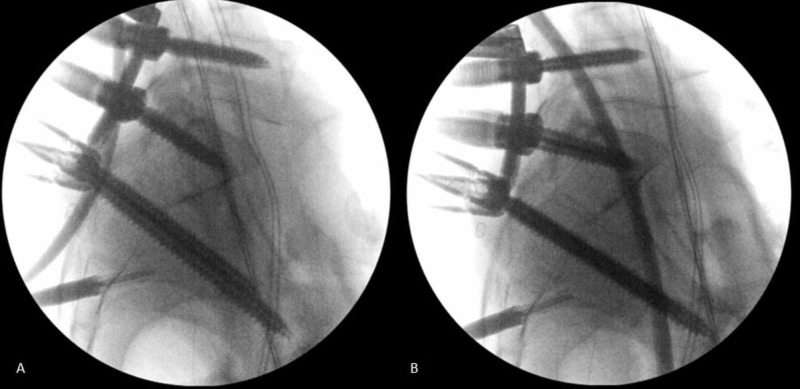
Multi-planar transverse, U-type, and vertical sacral fractures occur from high energy trauma or as pathologic fractures and often have associated neurologic and extremity injuries. Modern treatment algorithms fall into two broad categories: 1) percutaneous posterior pelvic fixation (iliosacral or transiliac-transsacral screws) or 2) lumbopelvic fixation. Posterior pelvic screw fixation is minimally invasive but typically requires restricted weight bearing until fracture union. In many cases, lumbopelvic fixation allows for a closed reduction and provides stability to allow full weight bearing immediately after surgery; however, this fixation is often removed in a second surgery after fracture healing. Lumbopelvic fixation was originally described as an open procedure, minimally invasive lumbopelvic fixation is a recent variation and has shown promising results with less morbidity. We present a case series of unstable U-type sacral fractures treated with minimally invasive lumbopelvic fixation with staged hardware removal to illustrate the advantages and complications associated with this new technique. Ten patients with U-type sacral fractures underwent minimally invasive lumbopelvic fixation from 2016 to 2019. Six patients underwent scheduled hardware removal an average of 3.5 (range 1.9-5.5) months after index surgery. Two patients did not undergo hardware removal due to short life expectancy and diagnosis of pathologic fractures. One patient was lost to follow-up. One patient had failed fracture reduction and went on to sacral malunion that required a late sacral extension osteotomy to restore her ability to stand upright. Final disposition of all nine patients with follow-up was normal standing upright posture and normal ambulation without assistive device. There were no late displacements on postoperative upright radiographs. Complex sacral fractures are a challenging injury that can be treated with percutaneous posterior pelvic or lumbopelvic fixation. Lumbopelvic fixation offers the advantages of closed reduction to restore pelvic incidence and immediate weight bearing but has greater surgical morbidity than percutaneous posterior pelvic fixation and often requires hardware removal. The morbidity of lumbopelvic fixation may be reduced with minimally invasive techniques. Minimally invasive lumbopelvic fixation is a treatment option to be considered for complex sacral fractures.
多平面横向、U型和垂直型骶骨骨折由高能量创伤引起或为病理性骨折,常伴有神经和肢体损伤。现代治疗方案主要分为两大类:1)经皮后路骨盆固定(髂骶或经髂-经骶螺钉)或2)腰骶骨盆固定。后路骨盆螺钉固定创伤小,但通常需要限制负重直至骨折愈合。在许多情况下,腰骶骨盆固定可实现闭合复位并提供稳定性,使患者术后可立即完全负重;然而,这种固定通常在骨折愈合后需二次手术取出。腰骶骨盆固定最初被描述为一种开放手术,微创腰骶骨盆固定是最近的一种术式,已显示出良好的效果且并发症较少。我们展示了一组采用微创腰骶骨盆固定并分期取出内固定物治疗不稳定U型骶骨骨折的病例系列,以说明这项新技术的优势和并发症。2016年至2019年,10例U型骶骨骨折患者接受了微创腰骶骨盆固定。6例患者在初次手术后平均3.5(范围1.9 - 5.5)个月接受了计划内的内固定物取出。2例患者因预期寿命短和病理性骨折诊断而未取出内固定物。1例患者失访。1例患者骨折复位失败,继而出现骶骨畸形愈合,需要后期行骶骨延长截骨术以恢复其直立能力。所有9例接受随访患者的最终情况是站立姿势正常,无需辅助装置即可正常行走。术后站立位X线片未见后期移位。复杂骶骨骨折是一种具有挑战性的损伤,可采用经皮后路骨盆或腰骶骨盆固定治疗。腰骶骨盆固定具有闭合复位以恢复骨盆倾斜度和立即负重的优势,但手术并发症比经皮后路骨盆固定更多,且通常需要取出内固定物。采用微创技术可降低腰骶骨盆固定的并发症。微创腰骶骨盆固定是复杂骶骨骨折可考虑的一种治疗选择。