Endo Yoko, Negishi Kousuke, Hirayama Kento, Suzuki Hitoshi, Shimizu Akira
Department of Analytic Human Pathology, Nippon Medical School.
Department of Nephrology, Tokyo-Shinagawa Hospital.
Medicine (Baltimore). 2019 Nov;98(45):e17870. doi: 10.1097/MD.0000000000017870.
Bevacizumab-an inhibitor of vascular endothelial growth factor-is effective against various advanced cancers. However, it is associated with the development of hypertension and high-grade proteinuria during thrombotic microangiopathy of the kidney. In addition, there are several reports of immunoglobulin A deposition in the glomeruli, but the etiology is unclear.
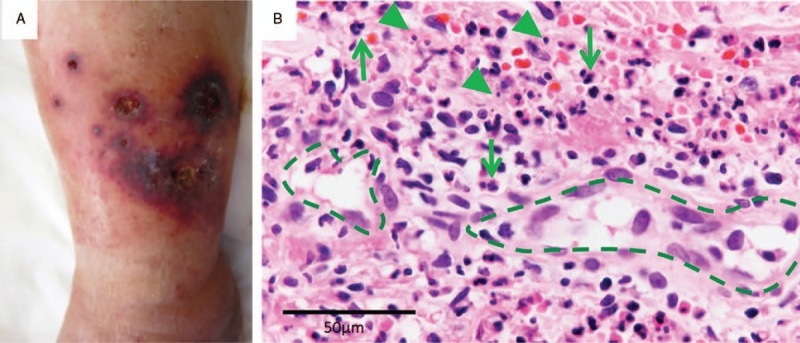
A 67-year-old Japanese man with metastatic rectal cancer underwent low anterior rectal resection, followed by treatment with bevacizumab and SOX (S-1 plus oxaliplatin). Six months later, the patient developed hematuria, nephrotic syndrome, and purpura.
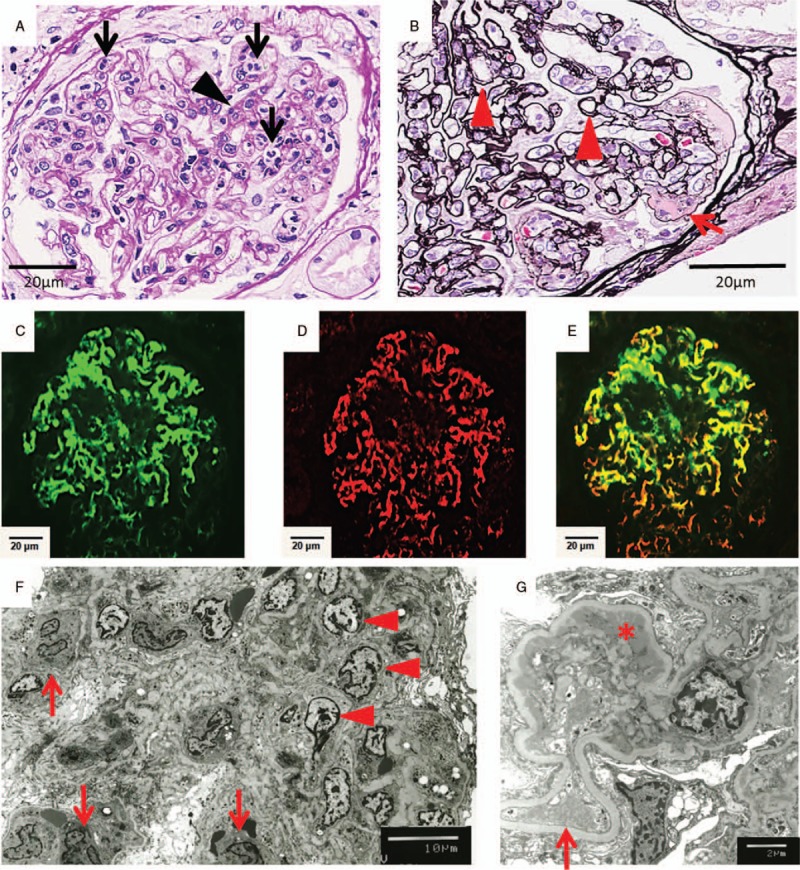
Renal biopsy revealed endocapillary proliferative glomerulonephritis. Immunofluorescence analyses showed granular mesangial deposition of galactose-deficient immunoglobulin A1. Skin biopsy revealed leukocytoclastic vasculitis.
We ceased bevacizumab treatment, while continuing the remaining chemotherapy regimen, as we suspected bevacizumab-induced nephropathy.
Proteinuria and purpura improved immediately after cessation of bevacizumab. We identified this as a case of bevacizumab-induced immunoglobulin A vasculitis with nephritis.
To our knowledge, this is the first case of bevacizumab-related immunoglobulin A vasculitis with nephritis, as evidenced by galactose-deficient immunoglobulin A1. When a patient's urine tests are abnormal during bevacizumab treatment, clinicians should consider not only thrombotic microangiopathy but also vasculitis.
贝伐单抗——一种血管内皮生长因子抑制剂——对多种晚期癌症有效。然而,它与肾血栓性微血管病期间高血压和重度蛋白尿的发生有关。此外,有几篇关于肾小球免疫球蛋白A沉积的报道,但病因尚不清楚。
一名67岁的日本转移性直肠癌男性患者接受了低位前直肠切除术,随后接受贝伐单抗和SOX(S-1加奥沙利铂)治疗。六个月后,患者出现血尿、肾病综合征和紫癜。
肾活检显示毛细血管内增生性肾小球肾炎。免疫荧光分析显示缺乏半乳糖的免疫球蛋白A1呈颗粒状系膜沉积。皮肤活检显示白细胞破碎性血管炎。
由于怀疑是贝伐单抗诱发的肾病,我们停止了贝伐单抗治疗,同时继续其余的化疗方案。
停用贝伐单抗后蛋白尿和紫癜立即改善。我们将此病例确定为贝伐单抗诱发的免疫球蛋白A血管炎伴肾炎。
据我们所知,这是首例由贝伐单抗引起的免疫球蛋白A血管炎伴肾炎病例,证据是缺乏半乳糖的免疫球蛋白A1。当患者在贝伐单抗治疗期间尿检异常时,临床医生不仅应考虑血栓性微血管病,还应考虑血管炎。