Department of Clinical Physiology, Karolinska Institute, and Karolinska University Hospital, Stockholm, Sweden.
Department of Physiology and Pharmacology, Section of Anesthesiology and Intensive Care Medicine, Karolinska Institutet, and Function Perioperative Medicine and Intensive Care, Karolinska University Hospital, Stockholm, Sweden.
J Cardiovasc Magn Reson. 2019 Nov 11;21(1):69. doi: 10.1186/s12968-019-0577-9.
Body position can be optimized for pulmonary ventilation/perfusion matching during surgery and intensive care. However, positional effects upon distribution of pulmonary blood flow and vascular distensibility measured as the pulmonary blood volume variation have not been quantitatively characterized. In order to explore the potential clinical utility of body position as a modulator of pulmonary hemodynamics, we aimed to characterize gravitational effects upon distribution of pulmonary blood flow, pulmonary vascular distension, and pulmonary vascular distensibility.
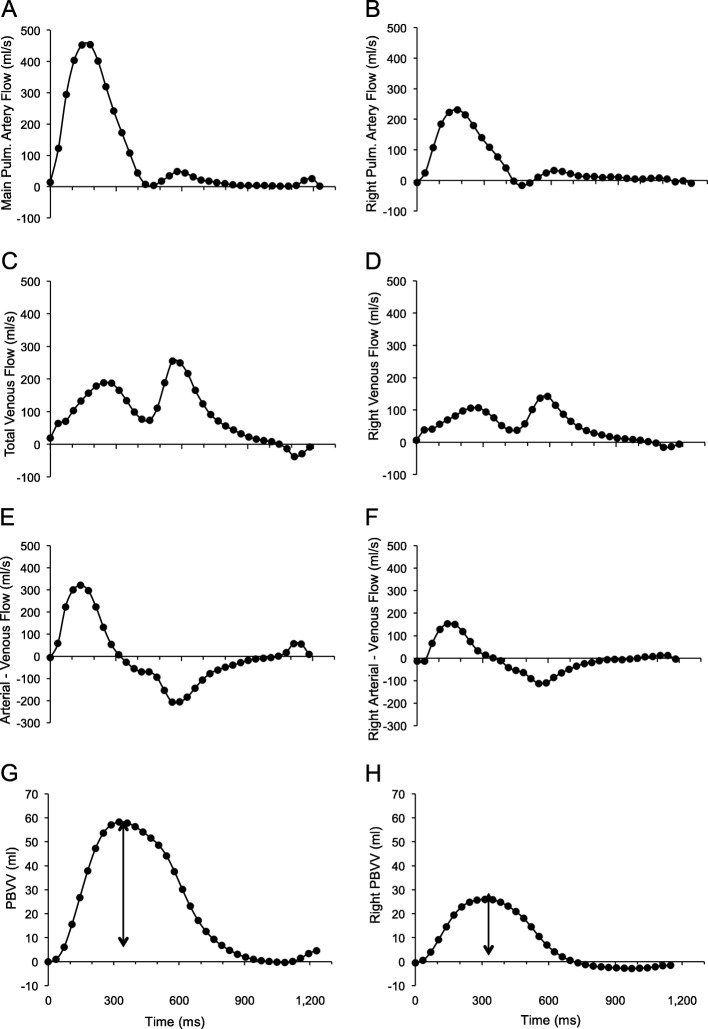
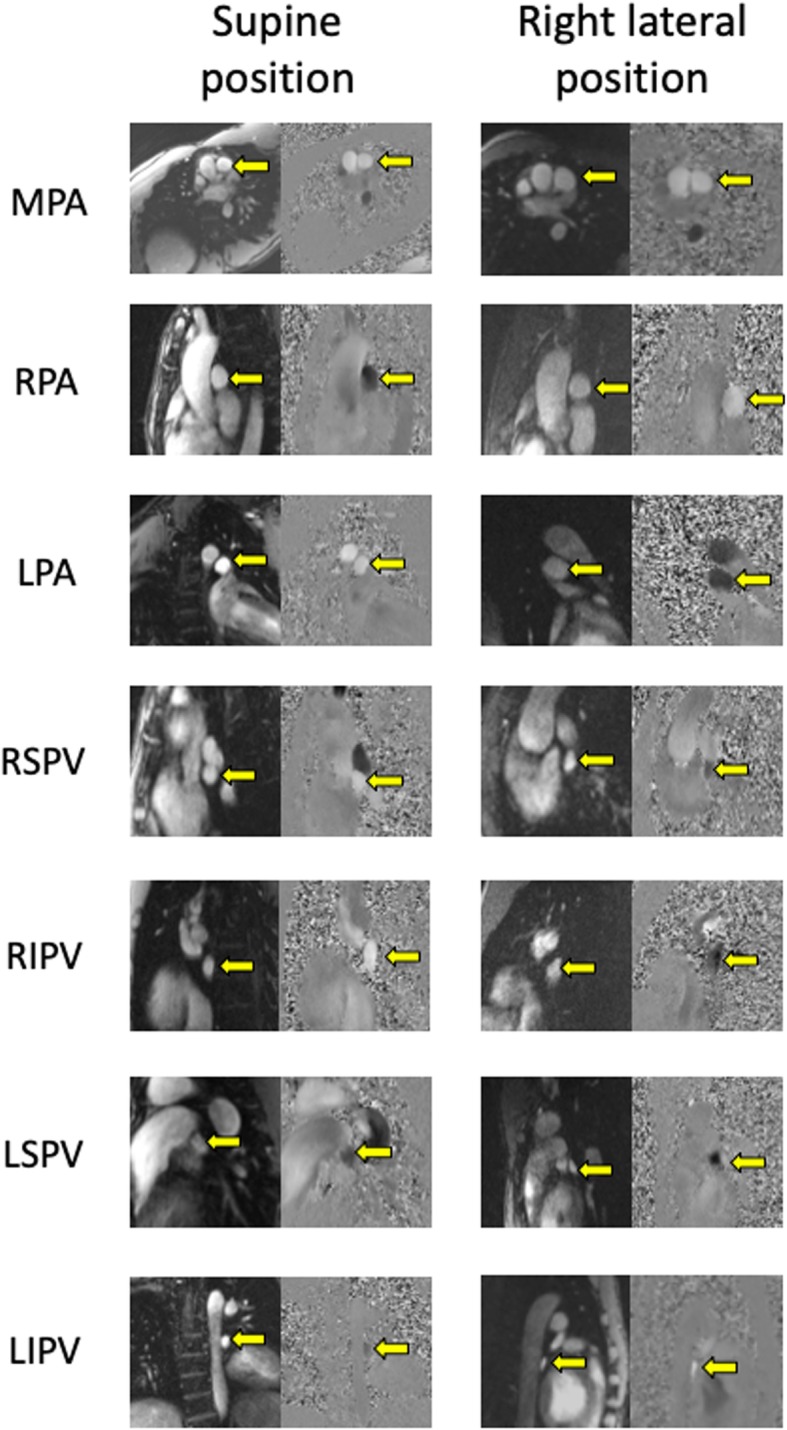
Healthy subjects (n = 10) underwent phase contrast cardiovascular magnetic resonance (CMR) pulmonary artery and vein flow measurements in the supine, prone, and right/left lateral decubitus positions. For each lung, blood volume variation was calculated by subtracting venous from arterial flow per time frame.
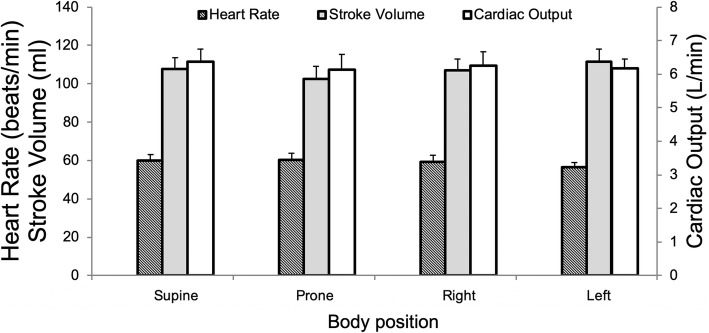
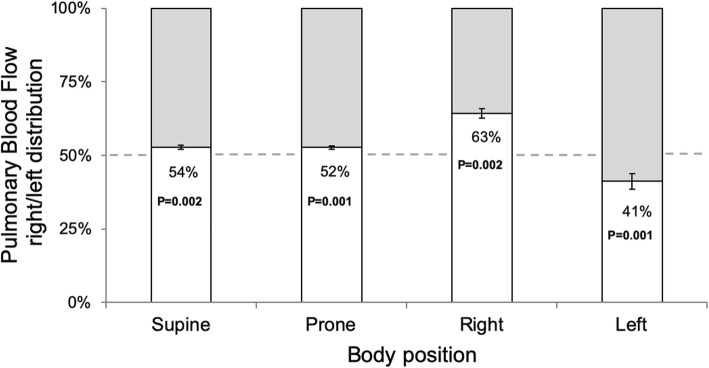
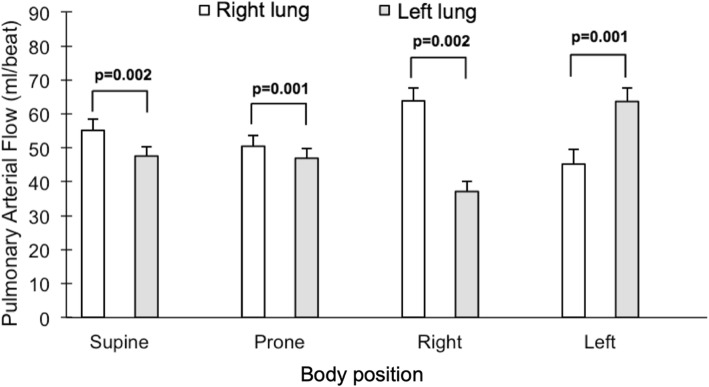
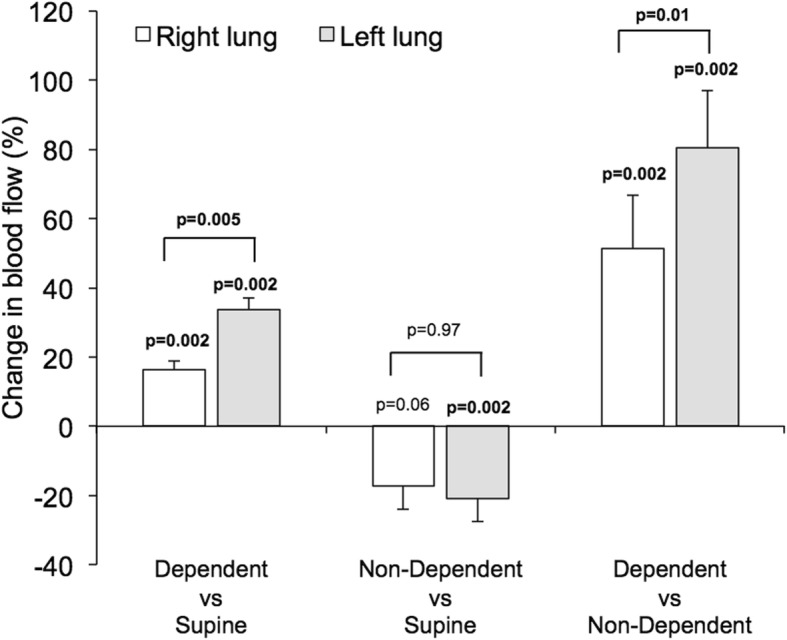
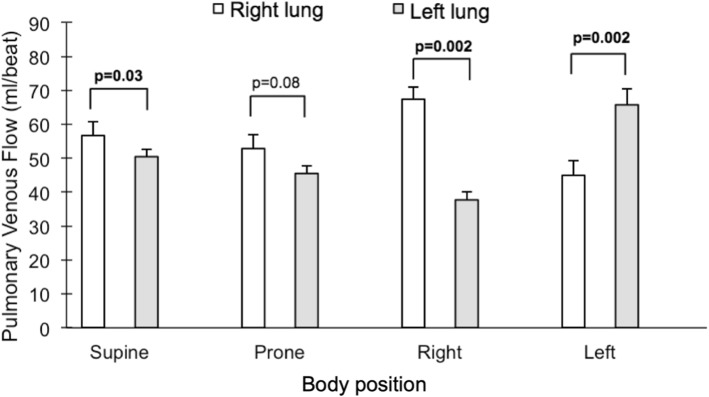
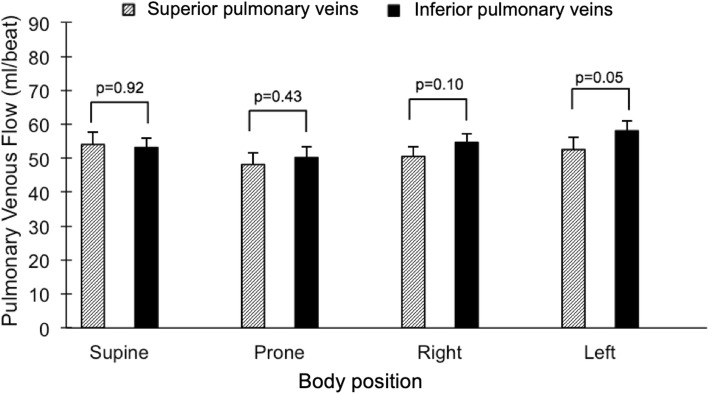
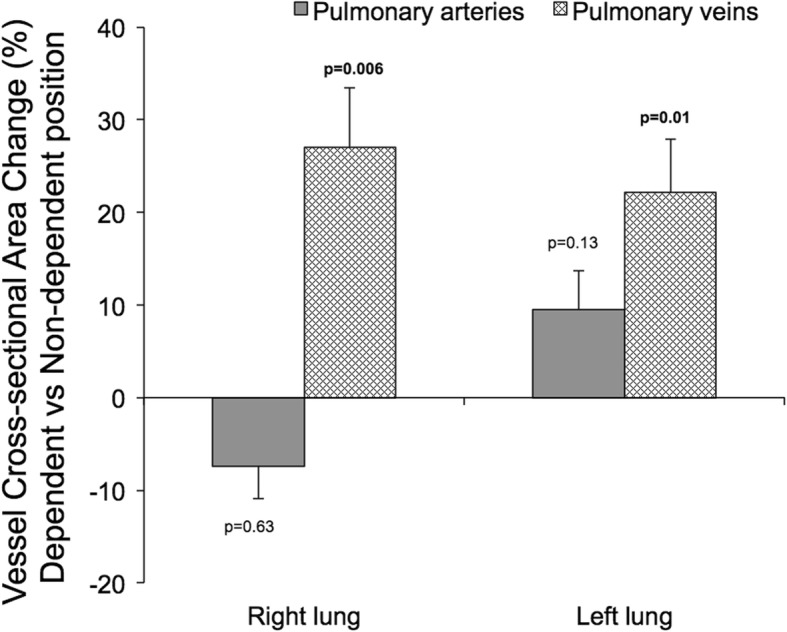
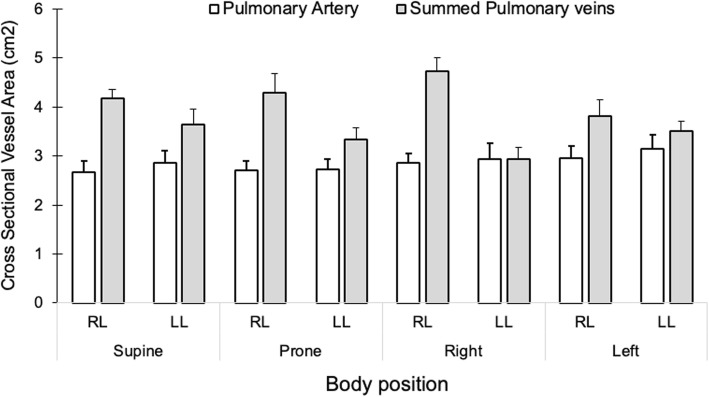
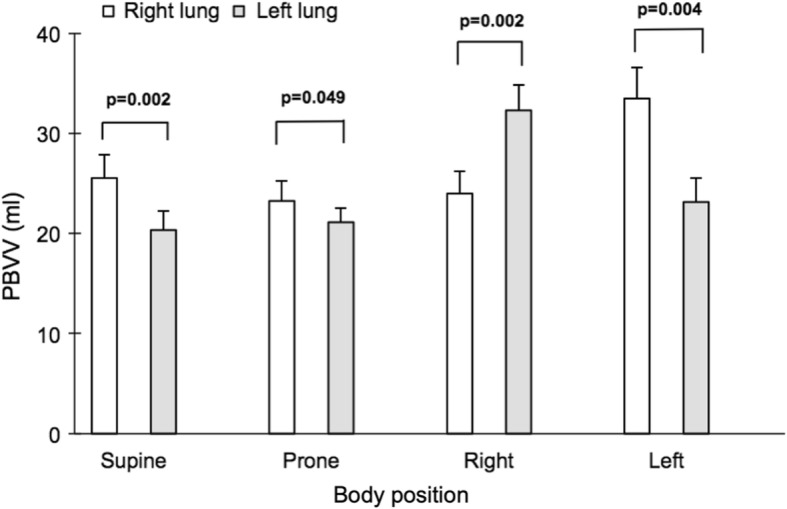
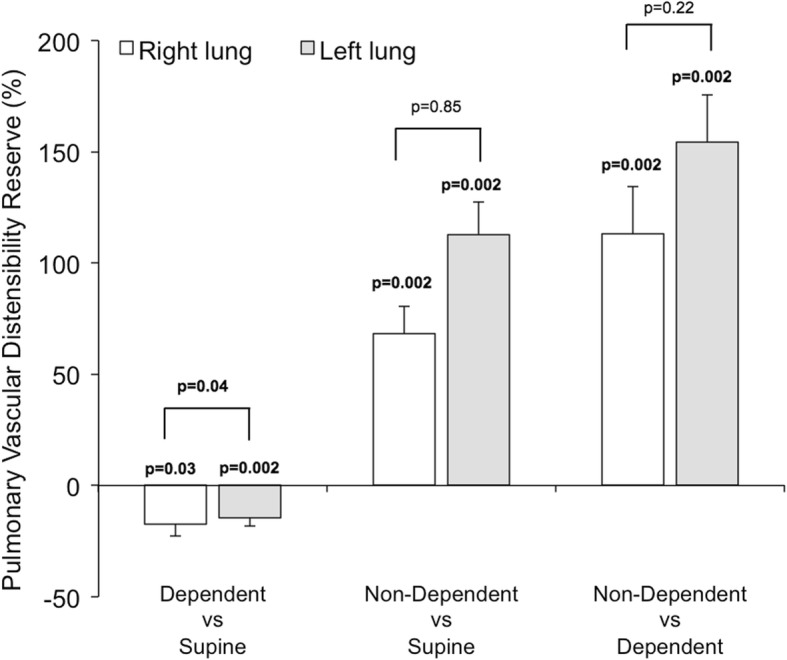
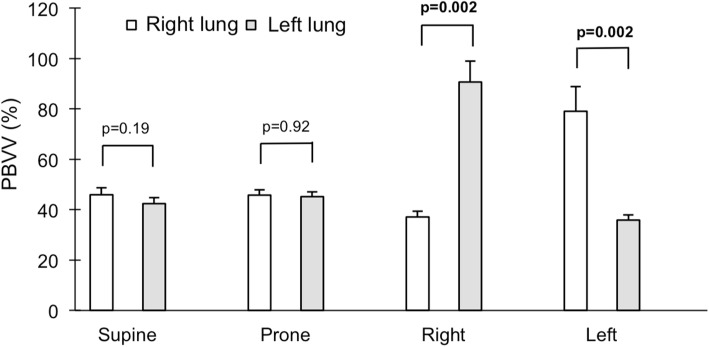
Body position did not change cardiac output (p = 0.84). There was no difference in blood flow between the superior and inferior pulmonary veins in the supine (p = 0.92) or prone body positions (p = 0.43). Compared to supine, pulmonary blood flow increased to the dependent lung in the lateral positions (16-33%, p = 0.002 for both). Venous but not arterial cross-sectional vessel area increased in both lungs when dependent compared to when non-dependent in the lateral positions (22-27%, p ≤ 0.01 for both). In contrast, compared to supine, distensibility increased in the non-dependent lung in the lateral positions (68-113%, p = 0.002 for both).
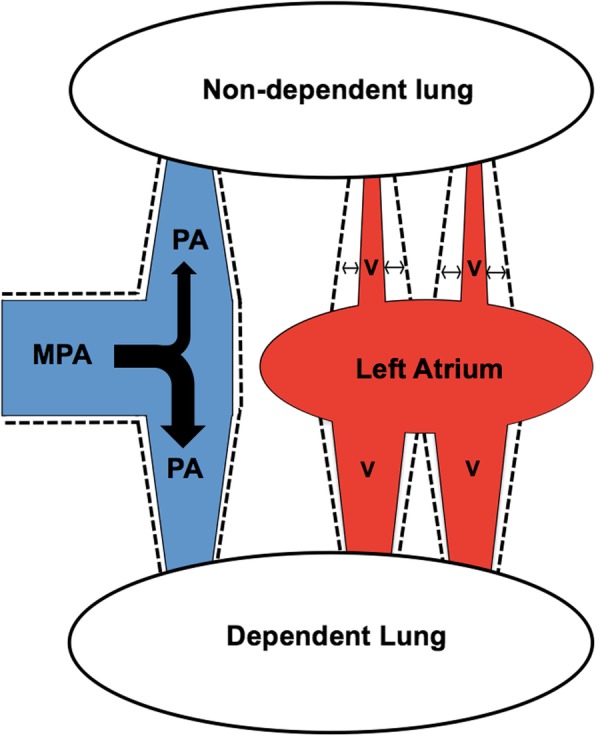
CMR demonstrates that in the lateral position, there is a shift in blood flow distribution, and venous but not arterial blood volume, from the non-dependent to the dependent lung. The non-dependent lung has a sizable pulmonary vascular distensibility reserve, possibly related to left atrial pressure. These results support the physiological basis for positioning patients with unilateral pulmonary pathology with the "good lung down" in the context of intensive care. Future studies are warranted to evaluate the diagnostic potential of these physiological insights into pulmonary hemodynamics, particularly in the context of non-invasively characterizing pulmonary hypertension.
在手术和重症监护期间,可以优化体位以实现肺通气/灌注匹配。然而,尚未对体位对肺血流量分布和血管扩张性(以肺血容量变化来衡量)的影响进行定量描述。为了探索体位作为肺血流动力学调节剂的潜在临床应用,我们旨在描述体位对肺血流量分布、肺血管扩张和肺血管扩张性的影响。
10 名健康受试者接受了仰卧位、俯卧位和右侧/左侧侧卧位下的相位对比心血管磁共振(CMR)肺动脉和静脉血流测量。对于每侧肺,通过从每个时间帧的动脉血流中减去静脉血流来计算血容量变化。
体位不改变心输出量(p=0.84)。仰卧位和俯卧位时,上肺静脉和下肺静脉之间的血流没有差异(p=0.92 和 p=0.43)。与仰卧位相比,侧卧时肺血流量增加到下垂肺(16-33%,p=0.002 均)。与非下垂相比,侧卧时两侧肺的静脉而非动脉的血管横截面积在下垂时增加(22-27%,p=0.01 均)。相比之下,与仰卧位相比,侧卧时非下垂肺的顺应性增加(68-113%,p=0.002 均)。
CMR 显示,在侧卧位时,血液从非下垂肺流向下垂肺,导致血流分布发生变化,静脉而非动脉的血容量发生变化。非下垂肺具有相当大的肺血管扩张储备能力,可能与左心房压力有关。这些结果支持在重症监护中对单侧肺病理患者采用“好肺在下”体位的生理基础。未来的研究需要评估这些对肺血流动力学的生理见解在诊断方面的潜力,特别是在无创性描述肺动脉高压方面。