Orces Carlos
Rheumatology, Laredo Medical Center, Laredo, USA.
Cureus. 2019 Sep 21;11(9):e5721. doi: 10.7759/cureus.5721.
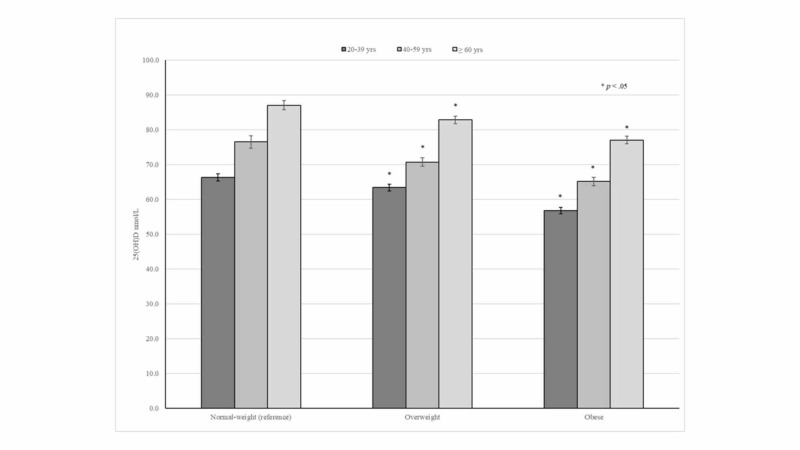
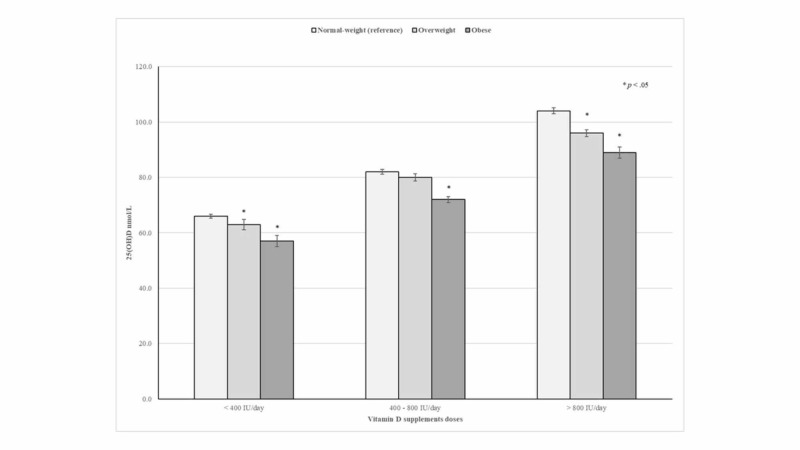
Background Obesity has been consistently associated with lower 25-hydroxyvitamin D (25(OH)D) concentrations. BMI status also has a major impact on 25(OH)D levels among vitamin D supplement users. In our cross-sectional study, we aimed to discuss the prevalence of vitamin D supplement use and its effect on 25(OH)D levels according to BMI status among US adults. Methods The present analysis was based on data from the National Health and Nutrition Examination Survey (NHANES) cycles 2011-2012 through 2013-2014. The prevalence of vitamin D supplement use according to BMI status among subjects aged 20 years and older by selected characteristics was analyzed. Logistic regression models were assembled to examine the independent association of BMI status and vitamin D supplement use. Similarly, general linear models were used to assess the effect of daily vitamin D supplementation doses (<400 IU, 400-800 IU, and >800 IU) on 25(OH)D concentrations according to BMI status. Results Of 10,076 participants with a mean age of 47.2 [standard error (SE): 0.4] years, 57.5% (SE: 1.7) of normal-weight and 63.5% (SE: 0.9) of obese subjects reported not taking vitamin D supplements over the previous 30 days. After adjustment for potential confounders, obese subjects were 1.3 times more likely to be nonusers of vitamin D supplements and were 24% less likely to take vitamin D supplements ≥400 IU/day compared with their normal-weight counterparts. In addition, significant differences in mean 25(OH)D levels of vitamin D supplementation doses were consistently seen across BMI categories. Indeed, obese and overweight participants taking >800 IU/day of vitamin D supplements had 15.5 and 8.1 nmol/L lower mean concentrations of 25(OH)D than their normal-weight counterparts on average, respectively. Conclusion Obese subjects had a lower prevalence of vitamin D supplement use compared with their normal-weight counterparts. This nutritional disparity may also contribute to low 25(OH)D concentrations seen in obesity. However, a daily vitamin D supplement intake between 400 IU and 800 IU appears to be adequate among obese subjects to achieve optimal 25(OH) levels.
肥胖一直与较低的25-羟基维生素D(25(OH)D)浓度相关。体重指数(BMI)状态对维生素D补充剂使用者的25(OH)D水平也有重大影响。在我们的横断面研究中,我们旨在探讨美国成年人中维生素D补充剂的使用 prevalence 及其根据BMI状态对25(OH)D水平的影响。方法:本分析基于2011 - 2012年至2013 - 2014年国家健康和营养检查调查(NHANES)的数据。按选定特征分析了20岁及以上受试者中根据BMI状态使用维生素D补充剂的 prevalence。组装逻辑回归模型以检验BMI状态与维生素D补充剂使用之间的独立关联。同样,使用一般线性模型根据BMI状态评估每日维生素D补充剂量(<400 IU、400 - 800 IU和>800 IU)对25(OH)D浓度的影响。结果:在10076名平均年龄为47.2[标准误差(SE):0.4]岁的参与者中,57.5%(SE:1.7)的正常体重者和63.5%(SE:0.9)的肥胖者报告在过去30天内未服用维生素D补充剂。在调整潜在混杂因素后,肥胖者不使用维生素D补充剂的可能性是正常体重者的1.3倍,且与正常体重者相比,每天服用维生素D补充剂≥400 IU的可能性低24%。此外,在不同BMI类别中,维生素D补充剂量的平均25(OH)D水平始终存在显著差异。确实,每天服用>800 IU维生素D补充剂的肥胖和超重参与者的25(OH)D平均浓度分别比正常体重者平均低15.5和8.1 nmol/L。结论:与正常体重者相比,肥胖者使用维生素D补充剂的 prevalence较低。这种营养差异也可能导致肥胖者中出现低25(OH)D浓度。然而,肥胖者中每天摄入400 IU至800 IU的维生素D补充剂似乎足以达到最佳的25(OH)水平。