Department of Surveillance, Prevention and Control of STIs, Ministry of Health of Brazil, HIV/AIDS and Viral Hepatitis, Brasilia, Brazil.
Tropical Medicine Foundation Heitor Vieira Dourado, Manaus, Brazil.
J Int AIDS Soc. 2019 Nov;22(11):e25397. doi: 10.1002/jia2.25397.
The relative efficacy of different antiretroviral (ART) regimens has been extensively evaluated in the context of clinical trials, using HIV viral load (VL) measurements at pre-specified timepoints after ART onset. However, data from real-life studies using combined longitudinal measurements of cumulative viraemia are scarce. This study aimed to address the independent effect of different ART regimens on HIV cumulative viraemia over the first 12 months after treatment initiation, using programmatic data from the Ministry of Health of Brazil.
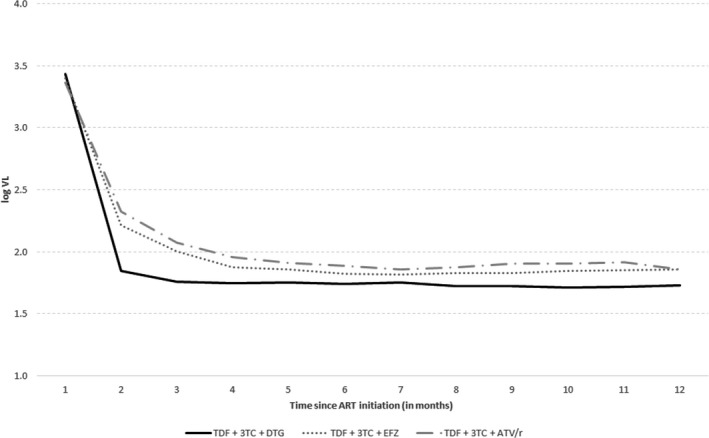
Retrospective cohort study analysing cumulative viraemia under the most frequently used ART regimens in Brazil (tenofovir, lamivudine and dolutegravir (regimen 1); tenofovir, lamivudine and efavirenz (regimen 2); tenofovir, lamivudine and ritonavir-boosted atazanavir (regimen 3)).
We included 112,243 patients >12 years old who received their first ART prescription between January 2014 and August 2017. Univariate analysis indicated that cumulative viraemia was significantly lower in patients receiving regimen 1 as compared with those receiving regimens 2 or 3 (p<0.0001 for both pairwise comparisons). In a multivariable analysis adjusted for age, sex, baseline T CD4+ counts and baseline HIV VL, ART regimen persisted with statistically significant effect on 12-month cumulative viraemia. The model predicted a 45-unit increase in log copy-days/mL cumulative viraemia for regimen 2 as compared with regimen 1, and a 70-unit increase in log copy-days/mL cumulative viraemia for regimen 3 as compared with regimen 1 (95%CI 41 to 49 and 61 to 79 respectively; p<0.001 for both comparisons). In models restricted to youths (13 to 24 years old) and female patients, ART regimen had similar effects. ART regimen with dolutegravir in association with a tenofovir-lamivudine backbone was superior to regimens containing efavirenz or boosted atazanavir in reducing HIV VL, as shown by cumulative viraemia over the first 12 months after treatment initiation. The superiority persisted even after adjusting the analysis for potential confounders.
Our findings could bring direct benefits to patients as suggested by lower viral replication during treatment, lower risk of HIV transmission, and a potential reduction in resistance mutations in the initial 12 months under ART.
不同抗逆转录病毒(ART)方案的相对疗效已在临床试验中得到广泛评估,使用 ART 开始后预定时间点的 HIV 病毒载量(VL)测量。然而,使用累积病毒血症的综合纵向测量的真实研究数据很少。本研究旨在利用巴西卫生部的规划数据,解决治疗开始后 12 个月内不同 ART 方案对 HIV 累积病毒血症的独立影响。
回顾性队列研究分析了巴西最常用的三种 ART 方案下的累积病毒血症(替诺福韦、拉米夫定和多替拉韦(方案 1);替诺福韦、拉米夫定和依非韦伦(方案 2);替诺福韦、拉米夫定和利托那韦增强的阿扎那韦(方案 3)。
我们纳入了 112243 名年龄大于 12 岁的患者,他们在 2014 年 1 月至 2017 年 8 月期间首次接受 ART 处方。单变量分析表明,与接受方案 2 或 3 的患者相比,接受方案 1 的患者累积病毒血症显著降低(两种方案比较的 p<0.0001)。在调整年龄、性别、基线 CD4+T 计数和基线 HIV VL 的多变量分析中,ART 方案对 12 个月累积病毒血症仍具有统计学意义的影响。该模型预测方案 2 与方案 1 相比,累积病毒血症对数拷贝数/mL 增加 45 个单位,方案 3 与方案 1 相比,累积病毒血症对数拷贝数/mL 增加 70 个单位(95%CI 分别为 41 至 49 和 61 至 79;两者比较均<0.001)。在仅包括青少年(13 至 24 岁)和女性患者的模型中,ART 方案也具有相似的效果。含有多替拉韦的 ART 方案与替诺福韦-拉米夫定联合方案优于含有依非韦伦或增强型阿扎那韦的方案,这一点从治疗开始后 12 个月内的累积病毒血症中可以看出。即使在对分析进行了潜在混杂因素调整后,这种优势仍然存在。
我们的研究结果可能会给患者带来直接的益处,因为治疗期间病毒复制减少、HIV 传播风险降低以及在最初 12 个月内 ART 中潜在的耐药突变减少。