Losurdo Giuseppe, Leandro Gioacchino, Ierardi Enzo, Perri Francesco, Barone Michele, Principi Mariabeatrice, Leo Alfredo Di
Section of Gastroenterology, Department of Emergency and Organ Transplantation, University "Aldo Moro", Piazza Giulio Cesare, B ari, Italy.
Gastroenterology Unit, National Institute of Research for Gastroenterology "Saverio De Bellis", Castellana Grotte, Bari, Italy.
J Neurogastroenterol Motil. 2020 Jan 30;26(1):16-28. doi: 10.5056/jnm19113.
BACKGROUND/AIMS: Small intestinal bacterial overgrowth (SIBO) diagnosis is usually based on non-invasive breath tests (BTs), namely lactulose BT (LBT) and glucose BT (GBT). However, divergent opinions and problems of parameter standardization are still controversial aspects. We aim to perform a meta-analysis to analyze diagnostic performance of LBT/GBT for SIBO diagnosis.
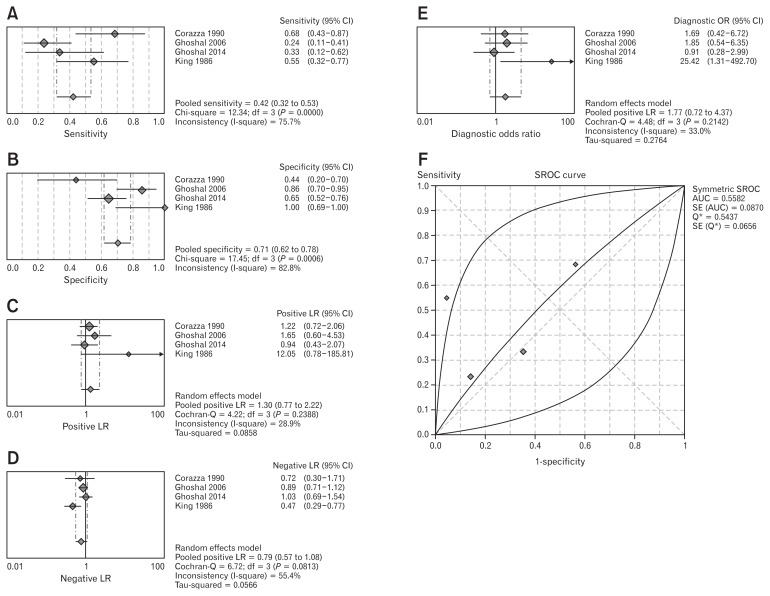
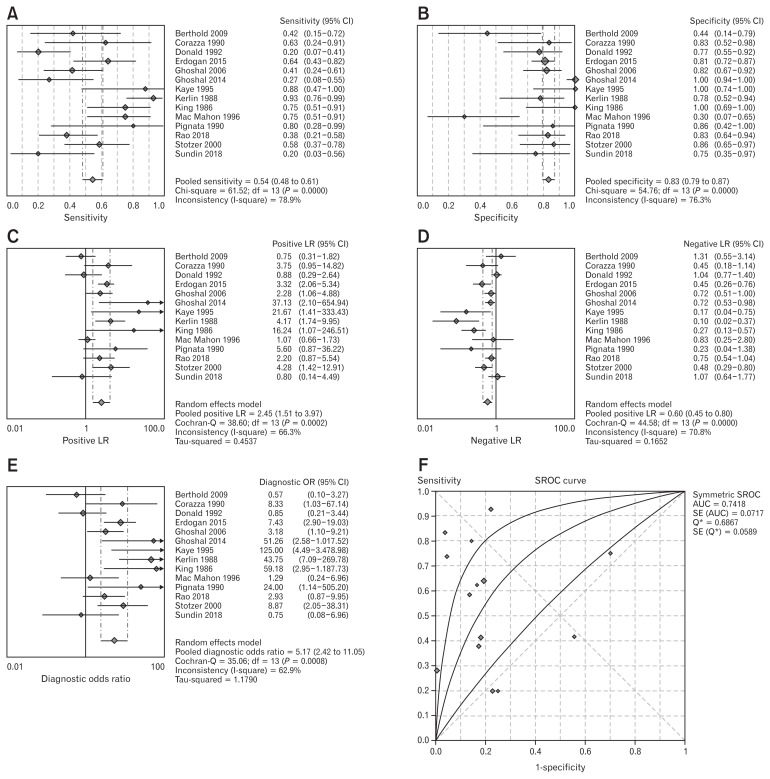
We searched in main literature databases articles in which SIBO diagnosis was achieved by LBT/GBT in comparison to jejunal aspirate culture (reference gold standard). We calculated pooled sensitivity, specificity, positive, and negative likelihood ratios and diagnostic odd ratios. Summary receiver operating characteristic curves were drawn and pooled areas under the curve were calculated.
We selected 14 studies. Pooled sensitivity of LBT and GBT was 42.0% and 54.5%, respectively. Pooled specificity of LBT and GBT was 70.6% and 83.2%, respectively. When delta over baseline cut-off > 20 H parts per million (ppm) was used, GBT sensitivity and specificity were 47.3% and 80.9%; when the cutoff was other than and lower than > 20 ppm, sensitivity and specificity were 61.7% and 86.0%. In patients with abdominal surgery history, pooled GBT sensitivity and specificity gave the impression of having a better performance (81.7% and 78.8%) compared to subjects without any SIBO predisposing condition (sensitivity = 40.6% and specificity = 84.0%).
GBT seems to work better than LBT. A cut-off of delta H2 expired other than and lower than > 20 ppm shows a slightly better result than > 20 ppm. BTs demonstrate the best effectiveness in patients with surgical reconstructions of gastrointestinal tract.
背景/目的:小肠细菌过度生长(SIBO)的诊断通常基于非侵入性呼气试验(BTs),即乳果糖呼气试验(LBT)和葡萄糖呼气试验(GBT)。然而,不同观点以及参数标准化问题仍是存在争议的方面。我们旨在进行一项荟萃分析,以分析LBT/GBT对SIBO诊断的性能。
我们在主要文献数据库中搜索了通过LBT/GBT与空肠抽吸物培养(参考金标准)相比进行SIBO诊断的文章。我们计算了合并敏感性、特异性、阳性和阴性似然比以及诊断比值比。绘制了汇总的受试者工作特征曲线并计算了曲线下的合并面积。
我们选择了14项研究。LBT和GBT的合并敏感性分别为42.0%和54.5%。LBT和GBT的合并特异性分别为70.6%和83.2%。当使用基线截止值变化>20 ppm时,GBT的敏感性和特异性分别为47.3%和80.9%;当截止值为其他且低于>20 ppm时,敏感性和特异性分别为61.7%和86.0%。在有腹部手术史的患者中,与没有任何SIBO易感因素的受试者相比(敏感性 = 40.6%,特异性 = 84.0%),合并的GBT敏感性和特异性表现更好(81.7%和78.8%)。
GBT似乎比LBT效果更好。基线截止值变化>20 ppm时,显示出比>20 ppm略好的结果。呼气试验在胃肠道手术重建患者中显示出最佳效果。