Global Digital Health Unit, Department of Primary Care and Public Health, Imperial College London, London, United Kingdom.
Infectious Diseases Section, Imperial College London, London, United Kingdom.
J Am Med Inform Assoc. 2020 Feb 1;27(2):274-283. doi: 10.1093/jamia/ocz186.
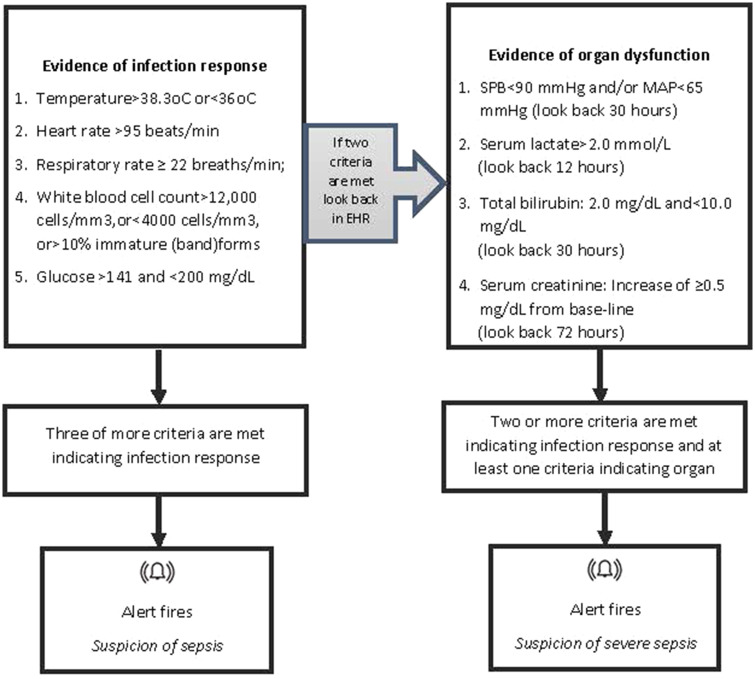
The study sought to determine the impact of a digital sepsis alert on patient outcomes in a UK multisite hospital network.
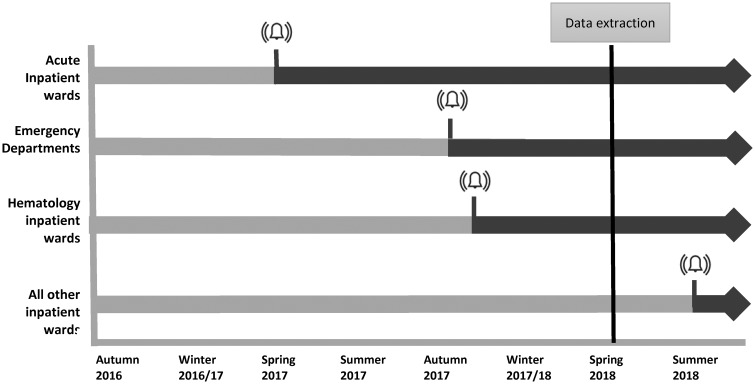
A natural experiment utilizing the phased introduction (without randomization) of a digital sepsis alert into a multisite hospital network. Sepsis alerts were either visible to clinicians (patients in the intervention group) or running silently and not visible (the control group). Inverse probability of treatment-weighted multivariable logistic regression was used to estimate the effect of the intervention on individual patient outcomes.
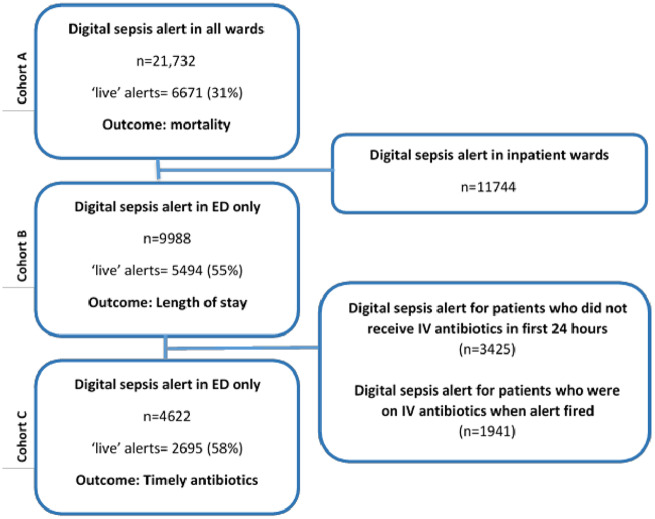
In-hospital 30-day mortality (all inpatients), prolonged hospital stay (≥7 days) and timely antibiotics (≤60 minutes of the alert) for patients who alerted in the emergency department.
The introduction of the alert was associated with lower odds of death (odds ratio, 0.76; 95% confidence interval [CI], 0.70-0.84; n = 21 183), lower odds of prolonged hospital stay ≥7 days (OR, 0.93; 95% CI, 0.88-0.99; n = 9988), and in patients who required antibiotics, an increased odds of receiving timely antibiotics (OR, 1.71; 95% CI, 1.57-1.87; n = 4622).
Current evidence that digital sepsis alerts are effective is mixed. In this large UK study, a digital sepsis alert has been shown to be associated with improved outcomes, including timely antibiotics. It is not known whether the presence of alerting is responsible for improved outcomes or whether the alert acted as a useful driver for quality improvement initiatives.
These findings strongly suggest that the introduction of a network-wide digital sepsis alert is associated with improvements in patient outcomes, demonstrating that digital based interventions can be successfully introduced and readily evaluated.
本研究旨在确定英国多地点医院网络中数字脓毒症警报对患者结局的影响。
利用数字脓毒症警报在多地点医院网络中的分阶段引入(无随机分组)进行自然实验。脓毒症警报对临床医生可见(干预组患者)或无声运行且不可见(对照组)。采用逆概率治疗加权多变量逻辑回归估计干预对个体患者结局的影响。
院内 30 天死亡率(所有住院患者)、延长住院时间(≥7 天)和急诊科发出警报的患者及时使用抗生素(≤60 分钟)。
警报的引入与死亡率降低相关(比值比,0.76;95%置信区间 [CI],0.70-0.84;n=21183),延长住院时间≥7 天的几率降低(比值比,0.93;95% CI,0.88-0.99;n=9988),需要使用抗生素的患者及时使用抗生素的几率增加(比值比,1.71;95% CI,1.57-1.87;n=4622)。
目前数字脓毒症警报有效的证据不一。在这项英国的大型研究中,数字脓毒症警报与改善结局相关,包括及时使用抗生素。目前尚不清楚警报的存在是否导致了改善的结局,或者警报是否作为质量改进举措的有用驱动力。
这些发现强烈表明,在整个网络范围内引入数字脓毒症警报与患者结局的改善相关,表明基于数字的干预措施可以成功引入并得到快速评估。